Choking in an infant demands a different response than choking in a child or adult. The anatomy of an infant’s airway is smaller, more fragile, and more easily damaged by techniques designed for older patients. The Infant Choking Algorithm gives you a structured, evidence-based sequence to identify a foreign-body airway obstruction in an infant under 1 year of age and act on it immediately with the correct technique.
The 2025 AHA and American Academy of Pediatrics guidelines updated the infant FBAO protocol to alternate 5 back blows with 5 chest thrusts, reinforcing that abdominal thrusts are never used in infants. This algorithm applies to any infant from birth through approximately 12 months of age, excluding newborns. Knowing the correct sequence and technique before you need it is what makes the difference when every second counts.

The Infant Choking Algorithm is the AHA and AAP-developed protocol for recognizing and managing foreign-body airway obstruction in infants under 1 year of age, excluding newborns. It applies in any setting, whether in a hospital, a clinic, a childcare environment, or a home. The algorithm classifies the obstruction as either mild or severe and guides your response based on that finding. Every action in the sequence is directed at one goal, which is removing the foreign body from the airway before the infant loses consciousness.
Liquids are the most common cause of airway obstruction in infants, though small objects and food fragments are also frequent causes. A severe obstruction that is not cleared within minutes leads to hypoxia, loss of consciousness, and cardiac arrest. Unlike older children and adults, infants cannot communicate distress verbally, which makes visual recognition of choking signs the most critical skill in the first moments of this emergency.
Responding to a choking infant requires precise technique and a calm, sequential approach. The steps below are specific to infants under 1 year of age. Do not apply child or adult choking techniques to an infant at any point in this sequence.
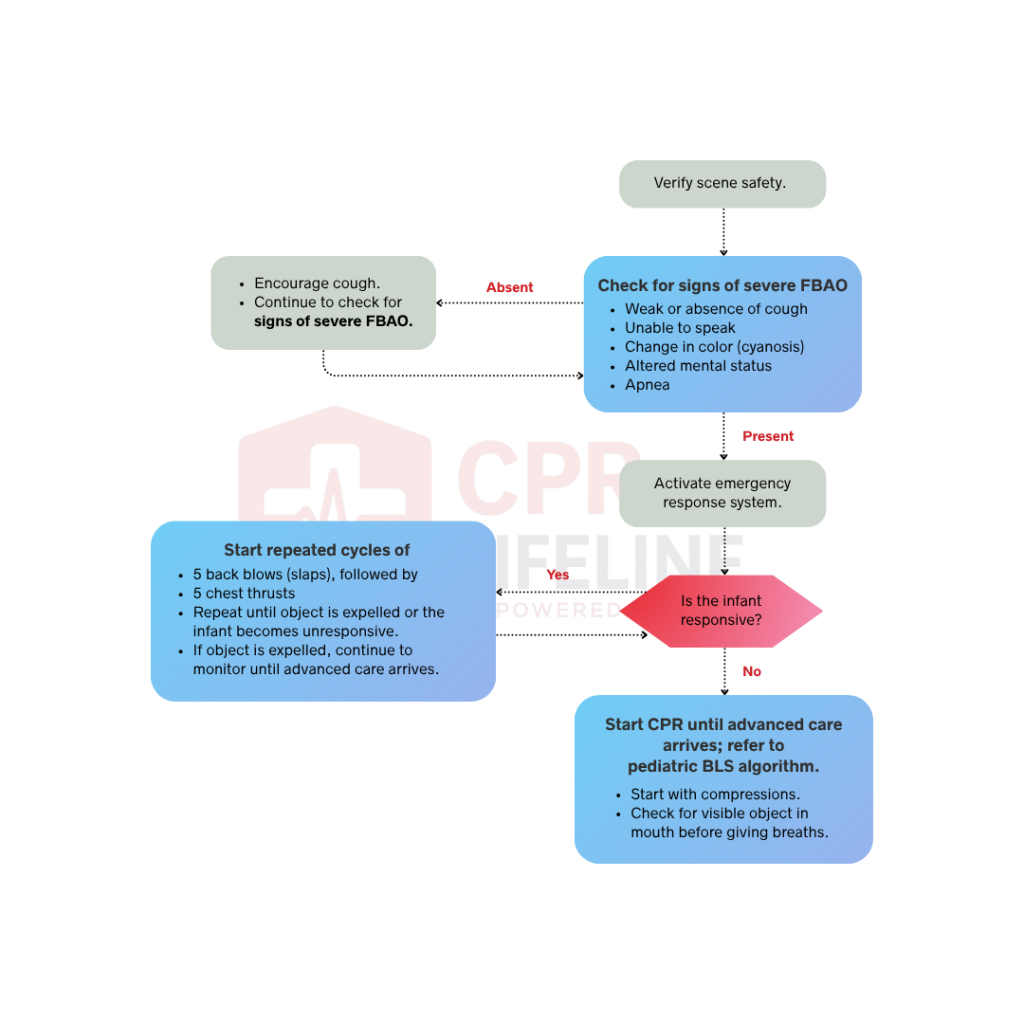
Before approaching, confirm the scene is safe. Once confirmed, assess the infant immediately. Unlike older children and adults, an infant cannot communicate distress verbally or display the universal choking sign. You must rely entirely on visual and auditory cues. Signs of choking in an infant include an inability to cry or make sounds, weak or absent breathing, a high-pitched sound or no sound at all while attempting to breathe, bluish discoloration of the lips or fingertips, and visible distress with wide eyes and an open mouth. After the scene is confirmed safe and choking has been identified, move to Step 2 to assess the severity of the obstruction.
The severity of the obstruction determines your entire next course of action. There are 2 possible findings at this stage.
An infant with a mild obstruction may cough, cry, or make audible sounds, indicating that air is still moving through the airway. Do not intervene physically in these cases and allow the infant to cough and monitor closely. A cough is the most effective way to clear a partial obstruction. If the cough weakens, the infant can no longer cry or make sounds, or breathing becomes visibly labored, the obstruction has progressed to severe. Move immediately to Step 3.
An infant with a severe obstruction cannot cough effectively, cry, or breathe. They may be silent, making a high-pitched sound, or showing visible signs of distress such as cyanosis or an open mouth with no air movement. Since these signs indicate a total airway blockage, you must not wait for the infant to become unresponsive. Move immediately to Step 3 without delay.
Hold the infant face down along your forearm with the head lower than the chest, ensuring the head and jaw are supported by your hand. Using the heel of your other hand, deliver five firm, distinct back blows between the shoulder blades. Do not strike the back of the head or the neck. After completing all five blows, you must check the mouth and remove the object only if it is visible and within easy reach. You should never perform a blind finger sweep, as this can push the object deeper into the airway. If the obstruction remains, you must move immediately to Step 4.
Turn the infant’s face up along your forearm, keeping the head lower than the chest. Place two fingers on the lower half of the sternum, just below the nipple line, and deliver five distinct downward chest thrusts. Each thrust must be firm and directed straight down toward the spine, providing enough force to potentially dislodge the obstruction.
After delivering all 5 chest thrusts, check the mouth again. If the object is visible and within easy reach, remove it. If the obstruction remains, return immediately to Step 3 and continue alternating cycles of 5 back blows and 5 chest thrusts.
Continue alternating between 5 back blows and 5 chest thrusts without stopping. Check the mouth after each set of back blows and remove the object immediately if it becomes visible and within easy reach. Never perform a blind finger sweep at any point during this cycle. If the object is expelled and the infant can cry, cough, or breathe normally, stop the cycle and monitor the infant. Encourage the caregiver to seek medical evaluation even if the infant appears fully recovered, as chest thrusts can cause internal injury that is not immediately visible. If the infant becomes unresponsive despite continued cycles, move immediately to Step 6.
Place the infant on their back on a firm, flat surface and call 911 if not already done. Begin chest compressions immediately following the Pediatric BLS Algorithm. Use the two-thumb encircling technique if a second rescuer is available, or the heel of one hand if you are alone. Compress at a rate of 100 to 120 per minute to a depth of approximately 1.5 inches. Each time you open the airway to deliver rescue breaths, look inside the mouth for the foreign object and remove it if it is visible and within easy reach. Continue CPR until the object is removed, the infant regains a pulse and begins breathing normally, or advanced care arrives and takes over.
Abdominal thrusts are contraindicated in infants because of the anatomical differences between an infant’s abdomen and that of an older child or adult. An infant’s abdominal organs, particularly the liver, are proportionally much larger relative to body size and sit higher in the abdominal cavity. They are also less protected by the rib cage. Delivering an inward and upward thrust to an infant’s abdomen carries a significant risk of lacerating the liver or damaging other abdominal organs, which can cause life-threatening internal bleeding.
Chest thrusts achieve the same physiological goal as abdominal thrusts without this risk. Both techniques work by generating a rapid increase in intrathoracic pressure that forces the foreign body upward and out of the airway. In an infant, chest thrusts deliver that pressure safely through the sternum rather than through the vulnerable abdominal organs. This is why the 2025 AHA and AAP guidelines specify chest thrusts exclusively for infants and why this distinction must never be confused with the child or adult protocol.
Infant, child, and adult choking share the same back blow first sequence but differ significantly in technique, thrust type, and CPR transition. The table below outlines the key differences.
Responding correctly to a choking infant requires precise positioning, controlled technique, and the ability to transition to CPR without hesitation. These are physical skills that cannot be developed through reading alone. The back blow and chest thrust sequence demands hands-on practice with an infant manikin before you encounter a real emergency, because without prior simulation training, providers make technique errors under pressure far more often.
BLS certification through the American Heart Association covers the full Infant Choking Algorithm alongside pediatric cardiac arrest management, rescue breathing, and CPR technique. Certification is valid for two years. If you are preparing for initial certification or an upcoming recertification, CPR Lifeline offers AHA-authorized BLS courses that incorporate the 2025 updated infant FBAO protocol with hands-on simulation.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
The 2025 AHA and AAP guidelines recommend alternating 5 back blows followed by 5 chest thrusts for any infant under 1 year of age with a severe airway obstruction. Hold the infant face down for back blows with the head lower than the chest, then turn them face up for chest thrusts. Repeat this cycle without stopping until the object is expelled or the infant becomes unresponsive. Never use abdominal thrusts on an infant under any circumstances.
An infant's abdominal organs, particularly the liver, are proportionally larger and less protected by the rib cage than in older children and adults. Delivering abdominal thrusts to an infant carries a significant risk of lacerating the liver or damaging other abdominal organs, causing life-threatening internal bleeding. Chest thrusts achieve the same goal of generating intrathoracic pressure to expel the foreign body without this risk.
Signs of choking in an infant include an inability to cry or make sounds, weak or absent breathing, a high-pitched sound or complete silence while attempting to breathe, and bluish discoloration of the lips or fingertips. Unlike older children and adults, an infant cannot display the universal choking sign. You must rely entirely on visual and auditory cues to identify the obstruction.
Place two fingers on the center of the chest on the lower half of the sternum, just below the nipple line. Deliver each thrust as a distinct downward compression directed straight toward the spine. Do not place your fingers on the very tip of the sternum or on the ribs. Correct finger placement ensures effective pressure generation without causing unnecessary injury.
Stop the intervention cycle and transition to CPR when the infant becomes unresponsive. Place the infant on their back on a firm, flat surface and begin chest compressions immediately following the Pediatric BLS Algorithm. Each time you open the airway to deliver rescue breaths, look inside the mouth for the foreign object and remove it if it is visible and within easy reach.
Yes. Any infant who experienced a choking episode should be evaluated by a medical provider, even if the object was successfully expelled and the infant appears fully recovered. Chest thrusts can cause internal injuries that are not immediately visible. A medical provider should assess the infant to rule out any injury caused by the intervention and confirm that the airway is fully clear.

Home | About Us | Classes | Locations | Blogs | FAQ’s | Group Training | Contact Us
Copyright © 2025 cprlifeline. All Rights Reserved. Powered by Splendour Group
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!