Pediatric cardiac arrest is rare, but it is survivable with fast, correct action. The pediatric Basic Life Support (BLS) algorithm gives you a clear, step-by-step framework to follow when a child or infant stops breathing or loses a pulse. Every second without intervention reduces the chance of survival, and hesitation during those first moments directly affects patient outcomes.
This algorithm covers how technique differs between infants and children, identifies the most common CPR errors, and answers the questions providers ask most often. Whether you are preparing for BLS certification or refreshing your clinical skills, this is the foundational knowledge you need to respond with confidence and accuracy.

The pediatric BLS algorithm is a structured response protocol developed by the American Heart Association (AHA). It defines what to assess, in what order, and what action to take based on each finding. This algorithm covers scene safety, responsiveness checks, pulse and breathing assessment, CPR technique, and AED use. It applies to infants under 1 year and children from age 1 to puberty. Technique and compression depth differ between these groups, but the decision-making sequence stays the same.
Most pediatric cardiac arrests follow a respiratory cause, not a primary cardiac event. A child typically loses oxygenation first, and the heart stops due to prolonged hypoxia rather than a primary arrhythmia. This is why high-quality ventilation carries as much weight in pediatric BLS as chest compressions.
The pediatric BLS algorithm follows a fixed sequence of assessments and actions where each step builds directly on the previous one. Skipping or rushing through any part of this protocol reduces the effectiveness of the entire response. By maintaining this structured approach, you ensure that every clinical intervention is delivered at the appropriate time to address the specific physiological needs of a child or infant.
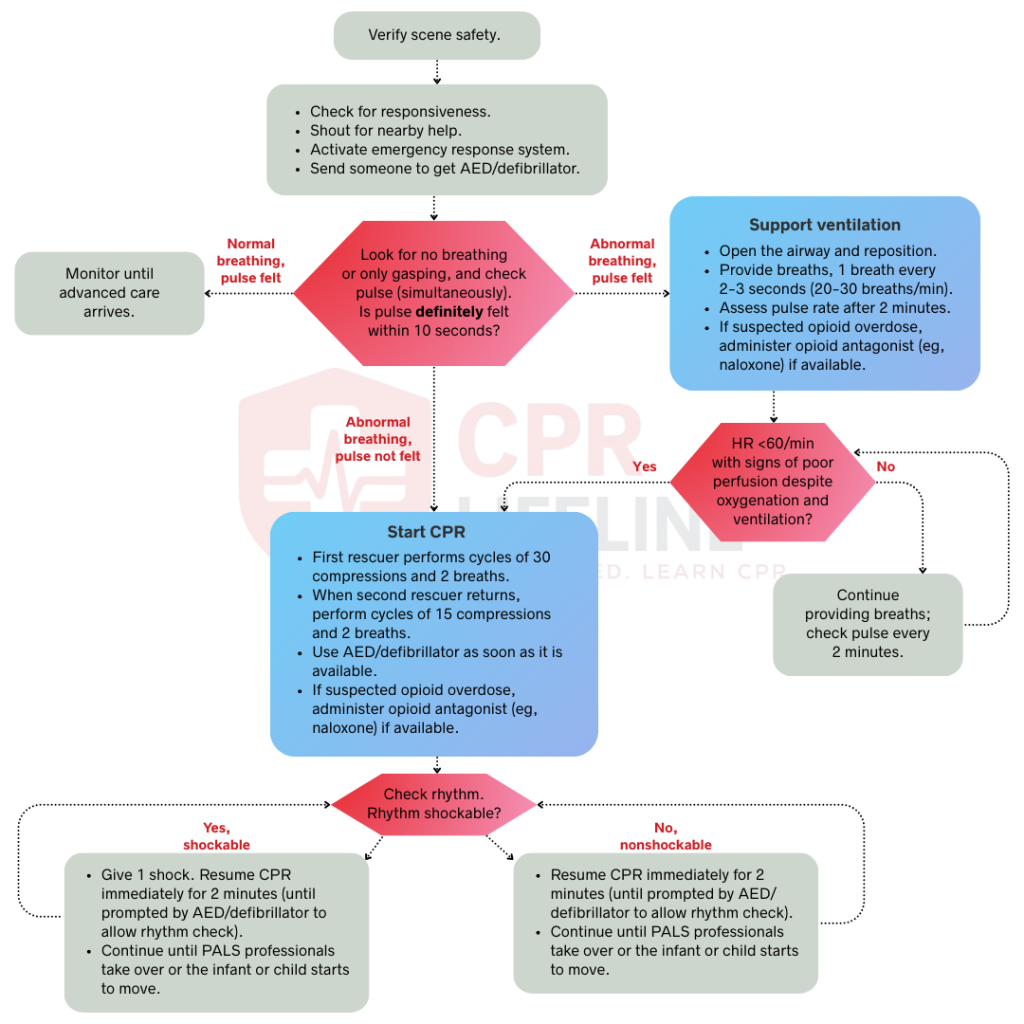
Before approaching the child, scan the environment for hazards. Look for traffic, unstable structures, or electrical dangers. Do not move toward the patient until the scene is safe, because an injured responder cannot help anyone. Put on gloves and a barrier device for rescue breathing if available.
Tap the child firmly on the shoulder and call out loudly. For an infant, flick the bottom of the foot. No response means you move immediately to the next steps. How you activate help depends on how many rescuers are present.
With two or more rescuers, one person begins CPR immediately while the other calls 911 and retrieves the AED. This parallel action removes any delay between starting compressions and activating EMS. With a single rescuer, the approach depends on whether the arrest was witnessed. For a witnessed arrest, call 911 and retrieve the AED before starting CPR. For an unwitnessed arrest, provide 2 minutes of CPR first, then leave to activate EMS. The 2-minute window gives the child a chance at return of spontaneous circulation before the rescuer steps away.
Place the child on a flat, firm surface and open the airway using a head-tilt chin-lift. For a suspected spinal injury, use a jaw thrust instead. Look for chest rise, and listen and feel for air movement at the mouth and nose. At the same time, palpate for a pulse. For children, use the carotid artery. For infants, use the brachial artery on the inner upper arm. Complete both assessments within 10 seconds or less.
Place the child in the recovery position if no spinal injury is suspected. This position keeps the airway open and prevents aspiration if vomiting occurs. For an infant, hold them on their side in your arms rather than placing them on the ground. Monitor breathing and pulse continuously. A pulse rate below 60 beats per minute with signs of poor perfusion requires immediate CPR, even if the child is breathing. Reassess every 2 minutes or sooner if the condition changes, and stay with the child until EMS arrives.
Deliver rescue breathing at 1 breath every 2 to 3 seconds, which equals 20 to 30 breaths per minute. Each breath should last 1 second and deliver just enough volume to produce a visible chest rise. Do not over-ventilate. Recheck the pulse every 2 minutes, and start CPR immediately if the pulse drops below 60 beats per minute with signs of poor perfusion such as pallor, mottling, or altered mental status.
Begin CPR immediately, starting with chest compressions. Deliver compressions at a rate of 100 to 120 per minute, pressing to a depth of at least one-third of the anterior-posterior chest diameter. This equals approximately 1.5 inches in infants and 2 inches in children. For children, place 1 to 2 hands on the lower half of the sternum regardless of rescuer count. Allow full chest recoil after every compression and do not lean on the chest between compressions. Keep all pauses in compressions under 10 seconds.
The compression technique and the ventilation ratio both depend on the number of rescuers present:
Apply AED pads as soon as the device is available and continue CPR without interruption until the AED is ready to analyze. For children under 8 years or under 25 kg, you should use pediatric pads or a pediatric dose attenuator. Use adult pads only when pediatric options are unavailable. For children, place one pad on the upper right chest and one on the lower left lateral chest. For infants, use anterior-posterior placement, one pad on the center of the chest and one on the center of the back, to avoid pad overlap. You must resume compressions immediately after a shock is delivered or if the device indicates that no shock is advised.
Deliver the initial shock at 2 J/kg and resume CPR immediately for 2 minutes without pausing to check the rhythm. You must reanalyze the rhythm after this 2-minute interval and increase the energy to 4 J/kg for the second shock if the rhythm remains shockable. Continue this cycle of 2-minute CPR followed by rhythm analysis and shock delivery to maintain consistent perfusion. For all subsequent shocks, use a dose of 4 J/kg or higher while ensuring you do not exceed 10 J/kg or the standard adult dose limit.
Resume CPR immediately and continue 2-minute cycles of high-quality compressions while reanalyzing the rhythm after each cycle. Throughout the resuscitation effort, you must actively search for and treat reversible causes by applying the H’s and T’s framework.
The algorithm structure is the same for both groups, but the technique differs based on size and physiology. The table below outlines the key differences.
Even well-trained healthcare providers make errors during pediatric resuscitation. A child’s small size, the stress of the moment, and the rarity of these emergencies all make it harder to perform the skills correctly. The three mistakes below are the most common ones in resuscitation research, and each one directly reduces the chance of survival. Knowing them before you are in that situation is what allows you to avoid them.
Compressions that do not reach the required depth fail to generate adequate coronary and cerebral perfusion pressure, marking one of the most frequent errors during pediatric CPR. You must achieve a minimum depth of one-third of the anterior-posterior chest diameter to maintain effective circulation. For most infants, that is about 1.5 inches, while for most children, it is about 2 inches. You should press firmly and deliberately to reach these targets and always allow for complete chest recoil after each compression. Incomplete recoil increases intrathoracic pressure and reduces venous return, which directly lowers cardiac output.
Over-ventilating a pediatric patient creates two clinical problems. First, by raising intrathoracic pressure and reducing cardiac output. Second, it interrupts the compression cycle and lowers the overall quality of the CPR effort. You should make sure each breath lasts exactly 1 second and produces only a visible chest rise to avoid delivering unnecessarily large tidal volumes. For small children and infants, a small puff of air is typically sufficient to achieve this goal. You must also avoid hyperventilation during advanced airway management by delivering 1 breath every 2 to 3 seconds without pausing chest compressions once the airway is secured.
While ventricular fibrillation is less common in children than in adults, its presence requires immediate action because every minute without defibrillation reduces survival by approximately 7% to 10%. You must apply the AED as soon as it becomes available rather than waiting to complete a full 2-minute CPR cycle. Attach the pads between compression cycles to minimize pauses and deliver the shock immediately once the AED advises. You should then resume compressions within 10 seconds of shock delivery without pausing to check for a pulse.
The pediatric BLS algorithm is not a framework you apply once and forget. It is a clinical skill that requires regular review and hands-on practice to execute correctly under pressure. The sequence covers scene safety, responsiveness, pulse and breathing assessment, high-quality CPR, and AED use. Each step depends on the one before it, and errors at any point weakens the whole rescue attempt. Familiarity with this algorithm is what separates a confident, effective response from a hesitant one.
If you are ready to build that confidence, CPR Lifeline offers AHA BLS certification in a blended learning format. You complete the knowledge portion online at your own pace, then finish with a hands-on skills session. It is structured for working professionals who need a flexible path to certification.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
The pediatric BLS algorithm is a step-by-step emergency response protocol developed by the American Heart Association. It guides rescuers through scene safety, responsiveness checks, pulse and breathing assessment, CPR, and AED use for children and infants in cardiac or respiratory arrest.
Use infant BLS techniques for children under 1 year of age. Apply child BLS techniques from age 1 until the onset of puberty. For adolescents who have reached puberty, you must apply adult BLS protocols to ensure the resuscitation efforts match the patient's physiological development.
Compress the chest at least one-third of its anterior-posterior diameter to ensure effective circulation. For most children aged 1 until the onset of puberty, this measurement is approximately 2 inches. For infants under 1 year of age, the target depth is approximately 1.5 inches.
Deliver compressions at a rate of 100 to 120 per minute for both infants and children. You should use a timer or metronome to stay within this specific range and maintain consistent perfusion. Rates that fall below 100 or exceed 120 per minute reduce the overall effectiveness of the CPR effort.
The compression-to-ventilation ratio depends on the number of rescuers present during the resuscitation effort. When only one rescuer is available, you should use a 30:2 ratio by providing 30 compressions followed by 2 breaths. If two or more rescuers are present, the ratio changes to 15:2 to prioritize oxygenation and ventilation for the pediatric patient.
Yes, you can use an AED on a child to restore a normal heart rhythm during cardiac arrest. For children under 8 years of age or weighing under 25 kg, you should use pediatric pads or a pediatric dose attenuator if they are available. You may use adult pads only when these pediatric options are not an option.
Deliver the first shock at a dose of 2 J/kg and increase to 4 J/kg for the second shock if the rhythm remains shockable. For all subsequent shocks, you should use a dose of 4 J/kg or higher while ensuring the energy does not exceed 10 J/kg or the standard adult dose limit.
Respiratory failure causes most pediatric cardiac arrests, often resulting from airway obstruction, drowning, severe asthma, or respiratory infections. Primary cardiac events such as ventricular fibrillation occur less frequently in children than in adults.

Home | About Us | Classes | Locations | Blogs | FAQ’s | Group Training | Contact Us
Copyright © 2025 cprlifeline. All Rights Reserved. Powered by Splendour Group
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!