
Not every fast heart rate in a child requires the same response. The PALS Tachycardia Algorithm gives you a structured, evidence-based sequence to identify the type of tachycardia, assess whether it is causing cardiopulmonary compromise, and select the right intervention based on both the rhythm and the patient’s clinical status. Developed by the American Heart Association, it guides your response from initial rhythm assessment through medication administration and synchronized cardioversion.
Tachycardia in a child becomes a clinical emergency when it produces hemodynamic instability. The algorithm is built around two key decision points: QRS duration and the presence or absence of cardiopulmonary compromise. Your answers to those two questions determine which pathway you follow and how quickly you need to act.

The PALS Tachycardia Algorithm is the AHA-developed protocol for identifying and managing tachycardia in pediatric patients. It applies to any child with a heart rate that is faster than expected for age and is causing or has the potential to cause cardiopulmonary compromise. The algorithm separates tachycardia into two broad categories based on QRS duration, narrow complex and wide complex, and further divides each category based on the patient’s hemodynamic stability.
The algorithm does not treat every fast heart rate as an emergency. Sinus tachycardia, which is the heart’s normal response to fever, pain, or hypovolemia, is managed by treating the underlying cause, not the rate itself. The PALS Tachycardia Algorithm focuses specifically on pathological tachycardias, primarily supraventricular tachycardia (SVT) and ventricular tachycardia (VT), where the rate itself is causing harm and requires direct intervention.
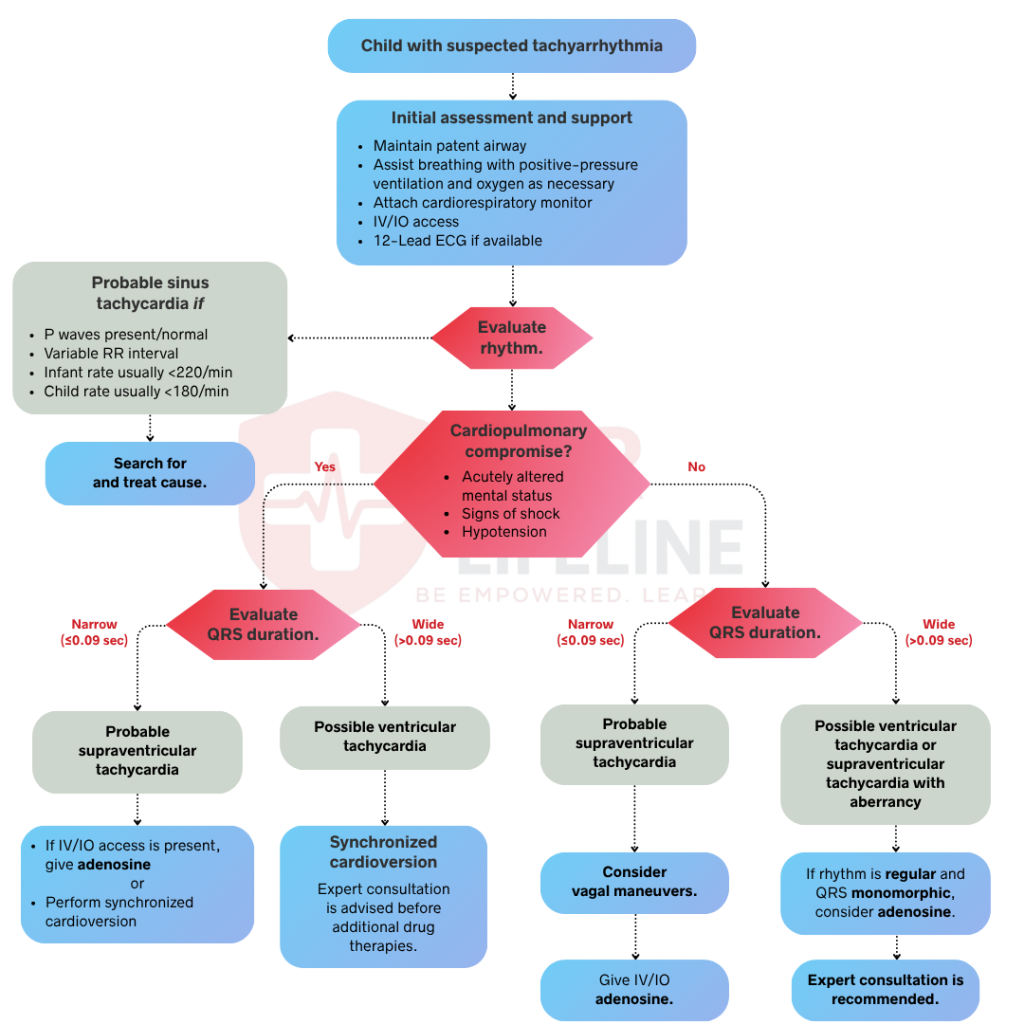
The PALS Tachycardia Algorithm follows a two-part decision structure. First, you assess the QRS duration to identify the rhythm type. Second, you assess hemodynamic stability to determine the urgency of intervention. In a team-based setting, several assessments occur simultaneously. Below is the full step-by-step breakdown, starting from the moment you identify a fast heart rate in a pediatric patient.
Tachycardia in a pediatric patient is a heart rate above the normal range for age. Your first task is to determine whether it is sinus tachycardia or a pathological rhythm. Sinus tachycardia is a compensatory response to fever, pain, or hypovolemia that presents with a gradual onset, a consistent P wave before each QRS, and a rate below 220 bpm in infants or 180 bpm in children. In contrast, SVT presents with an abrupt onset, a rate above those thresholds, and absent or abnormal P waves, while VT presents with a wide QRS and no consistent relationship between P waves and QRS complexes. You should treat sinus tachycardia by addressing the underlying cause rather than the rhythm itself.
Assess the patient for these 4 signs of cardiopulmonary compromise:
If none of these signs are present, the patient is stable, and you should move to Step 2. If any of the above signs are present, the patient is unstable and requires immediate intervention.
Once you confirm the tachycardia is pathological, assess the QRS duration on the monitor. This single measurement determines which treatment pathway you follow.
A narrow complex QRS is less than 0.09 seconds. Narrow complex tachycardia in a child is most likely SVT. A wide complex QRS is 0.09 seconds or greater. Wide complex tachycardia in a child is presumed VT until proven otherwise. Do not assume wide complex tachycardia is SVT with aberrant conduction in a pediatric patient. Treating presumed SVT with adenosine in a child with VT can cause hemodynamic deterioration.
If the QRS is narrow and the patient is stable, move to Step 3. If the QRS is narrow and the patient is unstable, move to Step 4. If the QRS is wide and the patient is stable, move to Step 5. If the QRS is wide and the patient is unstable, move to Step 6.
A stable patient with narrow complex tachycardia is most likely in SVT. You have time to attempt sequential interventions before escalating to cardioversion. Move through the following steps in order.
Vagal maneuvers are the first-line intervention for stable SVT. They work by stimulating the vagus nerve to slow conduction through the atrioventricular(AV) node, which can terminate SVT without medication. For infants and young children, apply ice to the face for 15 to 30 seconds without occluding the airway. For older children, instruct them to perform the Valsalva maneuver by bearing down or blowing through a narrow straw. Maintain continuous cardiac monitoring throughout the process. If the rhythm does not convert within one attempt, move immediately to adenosine without repeating the maneuver multiple times.
If vagal maneuvers fail to convert the rhythm, administer adenosine without delay. Adenosine is the first-line medication for SVT. It temporarily blocks AV node conduction and interrupts the re-entry circuit driving SVT. The initial dose is 0.1 mg/kg IV or IO, with a maximum first dose of 6 mg. Administer it as a rapid IV push followed immediately by a normal saline flush. If the first dose fails to convert the rhythm, double the dose to 0.2 mg/kg IV or IO, with a maximum second dose of 12 mg. Use the vein closest to the heart for administration. Peripheral veins in the hand or foot are less effective due to the drug’s extremely short half-life.
If adenosine fails to convert the rhythm or SVT recurs after conversion, proceed to synchronized cardioversion. Synchronized cardioversion delivers a shock timed to the R wave of the QRS complex, avoiding delivery during the vulnerable T wave period, which can precipitate VF. The initial energy dose is 0.5 to 1 J/kg. If the first attempt fails, increase to 2 J/kg. Provide sedation and analgesia before cardioversion in a conscious patient whenever possible. Do not delay cardioversion if the patient begins to show signs of hemodynamic instability. If the patient deteriorates at any point during Step 3, move immediately to Step 4.
An unstable patient with narrow complex tachycardia requires immediate synchronized cardioversion. Do not attempt vagal maneuvers or adenosine first. Set the defibrillator to synchronized mode and confirm it is marking the R wave on the monitor before delivering the shock. Start at 0.5 to 1 J/kg and increase to 2 J/kg if the first shock fails. Provide sedation and analgesia if the patient’s condition permits, but never delay the shock to obtain access or administer sedation in a critically unstable patient. Reassess perfusion immediately after cardioversion and consult pediatric critical care or a pediatric cardiologist without delay.
A stable patient with wide complex tachycardia is presumed to be in VT until proven otherwise. Do not treat this rhythm as SVT with aberrant conduction. Seek expert consultation with a pediatric cardiologist before initiating antiarrhythmic therapy. If consultation is available, administer amiodarone at 5 mg/kg IV or IO over 20 to 60 minutes as the preferred agent, or procainamide at 15 mg/kg IV or IO over 30 to 60 minutes as an alternative. Never administer both together, as the combination significantly increases the risk of dangerous arrhythmias. Monitor continuously during infusion and move immediately to Step 6 if the patient becomes unstable at any point.
An unstable patient with wide complex tachycardia requires immediate synchronized cardioversion. Do not attempt medications first. Set the defibrillator to synchronized mode and confirm it is marking the R wave before delivering the shock. Start at 0.5 to 1 J/kg and increase to 2 J/kg if the first shock fails. Provide sedation and analgesia if the patient’s condition permits, but never delay the shock in a critically unstable patient. If the rhythm deteriorates into pulseless VT or VF at any point, turn off synchronized mode, increase the energy to 2 J/kg, and transition immediately to the Pediatric Cardiac Arrest Algorithm. Reassess perfusion after each shock and consult pediatric critical care or a pediatric cardiologist without delay.
Once the tachycardia is converted or the patient is stabilized, consult a pediatric cardiologist if not already involved. Any child who requires cardioversion or antiarrhythmic therapy needs specialist evaluation to identify the underlying cause and prevent recurrence. Obtain a 12-lead ECG after conversion to document the baseline rhythm and identify any conduction abnormality. Continue continuous cardiac monitoring, maintain IV or IO access, and keep antiarrhythmic infusions running if initiated during resuscitation. Arrange transfer to a PICU for ongoing monitoring. If tachycardia recurs, re-enter the algorithm at Step 1 and reassess QRS duration and hemodynamic stability before selecting the next intervention.
Medications used in the PALS Tachycardia Algorithm have a specific indication, dose, and route. Knowing when to use each one and in what order is as important as knowing the dose.
The PALS Tachycardia Algorithm requires you to differentiate rhythm types, assess hemodynamic stability, and select the right intervention in a matter of seconds. These are high-stakes decisions that reading alone cannot prepare you for. Tachycardia scenarios are among the most complex in PALS training because the clinical presentation can shift rapidly from stable to unstable without warning.
PALS certification through the American Heart Association is required for physicians, nurses, paramedics, and respiratory therapists managing pediatric emergencies. Certification is valid for two years. If you are preparing for initial certification or an upcoming recertification, CPR Lifeline offers AHA-authorized PALS courses with pediatric-specific simulations covering every algorithm, including tachycardia, bradycardia, and cardiac arrest.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
Sinus tachycardia is a normal compensatory response to fever, pain, or hypovolemia. It has a gradual onset, a rate below 220 beats per minute in infants and below 180 in children, and a consistent P wave before each QRS. SVT has an abrupt onset, a rate above those thresholds, and absent or abnormal P waves. Sinus tachycardia is treated by addressing the underlying cause. SVT requires direct intervention with vagal maneuvers, adenosine, or cardioversion.
A narrow complex tachycardia has a QRS duration of less than 0.09 seconds and is most likely SVT in a pediatric patient. A wide complex tachycardia has a QRS duration of 0.09 seconds or greater and is presumed VT until proven otherwise. Do not assume wide complex tachycardia is SVT with aberrant conduction in a child. The treatment pathways for each are fundamentally different.
Vagal maneuvers are the first-line intervention for stable SVT. For infants and young children, apply ice to the face for 15 to 30 seconds. For older children, instruct them to perform the Valsalva maneuver. If vagal maneuvers fail, administer adenosine 0.1 mg/kg IV or IO as a rapid push. If adenosine fails, proceed to synchronized cardioversion at 0.5 to 1 J/kg.
The initial adenosine dose is 0.1 mg/kg IV or IO as a rapid push, with a maximum first dose of 6 mg. Administer it immediately, followed by a normal saline flush using the vein closest to the heart. If the first dose fails, double the dose to 0.2 mg/kg IV or IO, with a maximum second dose of 12 mg. Adenosine is not effective for VT and should never be used for wide complex tachycardia.
Synchronized cardioversion is used in two situations. First, for any unstable patient with tachycardia, regardless of QRS width, where hemodynamic compromise does not allow time for medications. Second, for a stable SVT that does not respond to vagal maneuvers and adenosine. The initial energy dose is 0.5 to 1 J/kg, increasing to 2 J/kg if the first shock fails. Always confirm the defibrillator is set to synchronized mode before delivering the shock.
No. Never administer amiodarone and procainamide together. The combination significantly increases the risk of dangerous arrhythmias, including torsades de pointes and refractory VF. Use amiodarone as the preferred first-line antiarrhythmic for stable VT. Use procainamide only as an alternative when amiodarone is unavailable or contraindicated, never in combination with it.

Home | About Us | Classes | Locations | Blogs | FAQ’s | Group Training | Contact Us
Copyright © 2025 cprlifeline. All Rights Reserved.
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!