
Pediatric cardiac arrest follows different rules than adult cardiac arrest. The causes, rhythms, and intervention priorities differ significantly, and applying adult protocols to a child directly worsens outcomes. The Pediatric Cardiac Arrest Algorithm gives you a structured, evidence-based sequence to manage cardiac arrest in infants and children from the first compression through rhythm-guided intervention and return of spontaneous circulation.
Children rarely experience cardiac arrest due to a primary cardiac cause. Pediatric cardiac arrest is most often the result of progressive respiratory failure or shock that goes untreated. This means early, high-quality CPR and airway management are the two most critical interventions in the first minutes. This algorithm guides you through both rhythm pathways, shockable and non-shockable, so your response is immediate, systematic, and clinically sound.

The Pediatric Cardiac Arrest Algorithm is the AHA-developed protocol for managing cardiac arrest in pediatric patients from infancy through adolescence. It applies to any unresponsive child, not breathing normally, and has no detectable pulse. The algorithm defines two distinct treatment pathways based on the cardiac rhythm identified on the monitor, shockable and non-shockable, and guides your response through each one.
The algorithm is built around continuous, high-quality CPR as the foundation of every intervention. Rhythm analysis, defibrillation, medication administration, and airway management all occur within the framework of minimizing interruptions to chest compressions. Every decision point in this algorithm is time-sensitive. Delays in any step reduce the likelihood of return of spontaneous circulation (ROSC) and survival with a favorable neurological outcome.
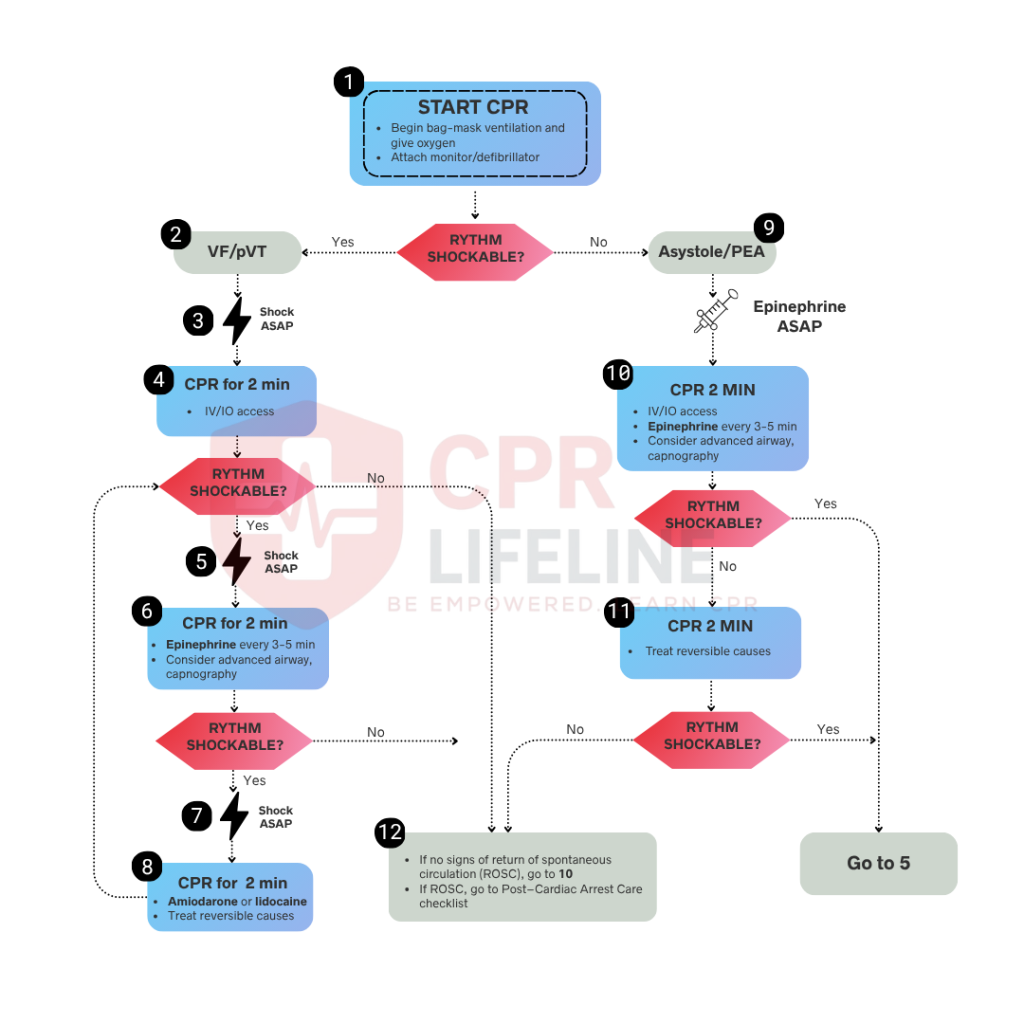
The Pediatric Cardiac Arrest Algorithm is divided into two rhythm-based pathways. Every step is built around minimizing interruptions to chest compressions. In a team-based setting, several interventions occur simultaneously. Below is the full step-by-step breakdown, starting from the moment cardiac arrest is confirmed in a pediatric patient.
Confirm cardiac arrest by assessing for unresponsiveness, absent or abnormal breathing, and the lack of a pulse within 10 seconds. If these signs are present, initiate chest compressions immediately. For infants, you should use the two-thumb encircling technique. For children, apply one or two hands to the lower half of the sternum. Compressions must be maintained at a rate of 100 to 120 per minute at a depth of at least one-third the anterior-posterior diameter of the chest, ensuring full recoil between each compression and limiting interruptions to less than 10 seconds. Maintain a 15:2 compression-to-ventilation ratio for two-rescuer teams or 30:2 for a single rescuer, and attach the cardiac monitor or defibrillator as soon as it is available without pausing compressions to prepare for rhythm analysis.
Once the monitor is attached, briefly pause compressions to analyze the rhythm. If you identify shockable rhythms such as ventricular fibrillation (VF) or pulseless ventricular tachycardia (pVT), provide immediate defibrillation and move to Step 3. If the monitor shows non-shockable rhythms, such as asystole or pulseless electrical activity (PEA), which do not respond to shocks, move directly to Step 4 to continue high-quality CPR and medication administration.
Ventricular fibrillation (VF) and pulseless ventricular tachycardia (pVT) both require immediate defibrillation. You should move through the following steps rapidly and without interruption to compressions wherever possible.
Deliver the first shock at 2 J/kg as soon as the defibrillator is charged, ensuring pads or paddles are applied to the child’s bare, dry chest with one placed below the right collarbone and the other on the left lateral chest below the armpit. After clearing all personnel from the patient and delivering the shock, resume CPR immediately without pausing for a pulse or rhythm check. Do not pause to assess rhythm until two minutes of CPR are complete.
Resume high-quality CPR immediately following the shock. Use the two-minute CPR cycle to establish IV or IO access if not already in place. IO access is both acceptable and preferred over repeated unsuccessful IV attempts.
If VF or pVT persists after the second shock, administer epinephrine 0.01 mg/kg IV or IO as soon as access is available and repeat the dose every 3 to 5 minutes throughout the resuscitation. Consider placing an advanced airway such as a supraglottic device or an endotracheal tube during this cycle to secure the respiratory tract. Once an advanced airway is in place, deliver continuous chest compressions at 100 to 120 per minute with asynchronous ventilations at a rate of 10 breaths per minute.
If VF or pVT persists after the third shock, administer an antiarrhythmic medication such as amiodarone at 5 mg/kg IV or IO as a bolus. You may repeat this dose up to two times for refractory VF or pVT, or you may use lidocaine as an acceptable alternative at 1 mg/kg IV or IO. Continue the cycle of CPR, rhythm analysis, shock delivery, and medication administration until ROSC is achieved, the rhythm converts, or a qualified provider stops resuscitation efforts.
Asystole and PEA do not respond to defibrillation, so your focus must remain on continuous high-quality CPR and early epinephrine administration while you simultaneously identify and treat reversible causes.
Begin or continue high-quality CPR immediately and use the first two-minute cycle to establish IV or IO access if it is not already in place. You must not interrupt compressions to obtain this access because maintaining coronary perfusion is the priority. Since delays in medication delivery can decrease the chance of survival, IO access is acceptable and preferred over repeated failed IV attempts.
Administer epinephrine 0.01 mg/kg IV or IO as soon as access is established. Repeat every 3 to 5 minutes throughout the resuscitation. Do not delay the first dose. Early epinephrine administration improves coronary and cerebral perfusion pressure during CPR and increases the likelihood of ROSC.
Simultaneously investigate and treat reversible causes using the Hs and Ts framework. The Hs include hypoxia, hypovolemia, hypothermia, hydrogen ion excess, and electrolyte abnormalities. The Ts include tension pneumothorax, cardiac tamponade, toxins, and thrombosis. Continue CPR with rhythm checks every two minutes. If the rhythm converts to a shockable rhythm at any point, move immediately to Step 3. If ROSC is achieved, move to Step 5.
If VF or pVT persists after the third shock, administer an antiarrhythmic medication such as amiodarone at 5 mg/kg IV or IO as a bolus. You may repeat this dose up to two times for refractory VF or pVT, or you may use lidocaine as an acceptable alternative at 1 mg/kg IV or IO. Continue the cycle of CPR, rhythm analysis, shock delivery, and medication administration until ROSC is achieved, the rhythm converts, or a qualified provider stops resuscitation efforts.
ROSC is confirmed when a palpable pulse returns and the monitor shows an organized rhythm. At this point, your focus shifts immediately to post-cardiac arrest care. Titrate oxygen to maintain SpO2 between 94 and 99 percent to avoid both hypoxia and hyperoxia. Maintain age-appropriate blood pressure with fluid boluses or vasoactive infusions as needed. Check glucose and correct hypoglycemia immediately. Obtain a 12-lead ECG to identify any underlying arrhythmia or conduction abnormality.
Do not hyperventilate the patient after ROSC. Target a PaCO2 of 35 to 45 mmHg, as hypocapnia causes cerebral vasoconstriction and worsens neurological outcomes. Avoid hyperthermia and consider targeted temperature management in comatose patients. Consult pediatric critical care immediately and arrange transfer to a PICU for ongoing monitoring and management.
The Hs and Ts framework is a systematic tool for identifying and treating reversible causes of cardiac arrest. In pediatric patients, addressing these causes during resuscitation is as important as CPR and defibrillation. A cardiac arrest that does not respond to standard interventions almost always has an underlying reversible cause driving it. There are 5 Hs and 4 Ts in pediatric cardiac arrest management.
Three medications are used in the Pediatric Cardiac Arrest Algorithm. Each has a specific indication, dose, and route. Knowing when and how to administer each one without interrupting CPR is a core skill in pediatric resuscitation.
Pediatric and adult cardiac arrest share the same algorithm structure but differ significantly in cause, rhythm distribution, compression technique, and drug dosing. Applying adult protocols to a pediatric patient without adjustment directly reduces survival outcomes. The table below outlines the key differences.
The Pediatric Cardiac Arrest Algorithm demands split-second decisions, weight-based drug dosing, and age-specific compression techniques that cannot be learned through reading alone. Pediatric cardiac arrest is the highest-stakes scenario in PALS training, and the gap between knowing the algorithm and executing it correctly under pressure is significant. Simulation-based training is the only way to close that gap before you face it in a real clinical setting.
PALS certification through the American Heart Association is required for physicians, nurses, paramedics, and respiratory therapists managing pediatric emergencies. Certification is valid for two years. If you are preparing for initial certification or an upcoming recertification, CPR Lifeline offers AHA-authorized PALS courses with pediatric-specific simulations covering every algorithm, including cardiac arrest, bradycardia, and septic shock.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
Respiratory failure and shock are the most common causes of cardiac arrest in children. Unlike adults, children rarely arrest from a primary cardiac event. This is why early airway management and oxygenation are the highest priorities in pediatric resuscitation. Preventing cardiac arrest by treating respiratory failure or shock before the pulse is lost is far more effective than managing arrest after it occurs.
Compress to a depth of at least one-third the anterior-posterior diameter of the chest. This equals approximately 1.5 inches for infants and 2 inches for children. Allow full chest recoil between each compression and keep all interruptions under 10 seconds.
Both are used for refractory VF or pVT that persists after the third shock. Amiodarone is the first-line antiarrhythmic at 5 mg/kg IV or IO, repeatable up to two times. Lidocaine is an acceptable alternative at 1 mg/kg IV or IO when amiodarone is unavailable or contraindicated. Neither drug is used for non-shockable rhythms.
The two shockable rhythms in pediatric cardiac arrest are ventricular fibrillation (VF) and pulseless ventricular tachycardia (pVT). Both require immediate defibrillation followed by two minutes of CPR before the next rhythm check. Asystole and PEA are non-shockable rhythms and do not respond to defibrillation.
The first shock dose for pediatric defibrillation is 2 J/kg. If VF or pVT persists, increase subsequent shocks to 4 J/kg. The maximum single shock dose is 10 J/kg or the adult maximum dose, whichever is lower. Resume CPR immediately after each shock without pausing to check for a pulse.
The 2025 AHA guidelines eliminated the two-finger compression technique for infant CPR. The two-thumb encircling technique is now the recommended method for all infant compressions regardless of rescuer number. The guidelines also reinforced the importance of avoiding both hypoxia and hyperoxia after ROSC, with a target SpO2 of 94 to 99 percent, and emphasized early epinephrine administration in non-shockable rhythms.
PALS certification is valid for two years. Given the complexity of pediatric resuscitation and the low frequency of pediatric cardiac arrest in most clinical settings, skills refreshers between certification cycles are strongly recommended to maintain competency.

Home | About Us | Classes | Locations | Blogs | FAQ’s | Group Training | Contact Us
Copyright © 2025 cprlifeline. All Rights Reserved. Powered by Splendour Group
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!