
Bradycardia in a child is not always an emergency, but it can become one fast. The Pediatric Advanced Life Support (PALS) Bradycardia Algorithm gives you a structured, evidence-based sequence to assess and manage a child with a slow heart rate. Developed by the American Heart Association (AHA), it helps you determine whether the bradycardia is causing cardiopulmonary compromise and what action to take based on that finding.
Unlike adult bradycardia, pediatric bradycardia is most often caused by hypoxia, not a primary cardiac problem. This completely changes how you respond. This algorithm guides you from initial assessment through airway support, medication administration, and pacing, so you are never guessing the next step when a child’s condition is deteriorating.

The PALS Bradycardia Algorithm is the AHA-developed protocol for identifying and treating bradycardia in pediatric patients. It applies to infants, children, and adolescents up to 18 years of age. This algorithm defines bradycardia as a heart rate below 60 beats per minute in a child who is showing signs of poor perfusion, regardless of the exact number on the monitor.
The algorithm is built around one central question: Is the slow heart rate causing cardiopulmonary compromise? The answer to that question determines every step that follows. A child with bradycardia but no signs of compromise is managed differently from one who is deteriorating. Knowing how to make that distinction quickly, and act on it correctly, is the core skill this algorithm teaches.
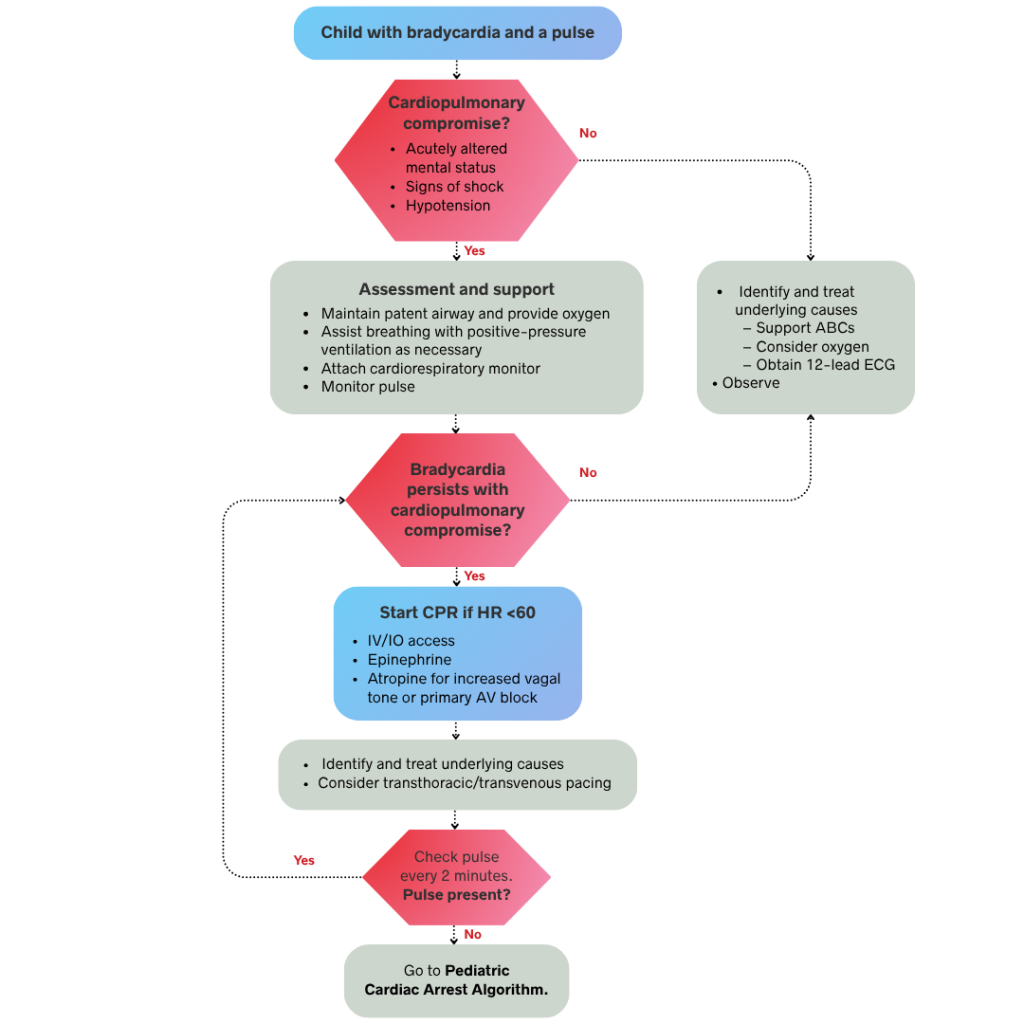
The PALS Bradycardia Algorithm follows a decision-based sequence. Each step depends on your clinical findings from the previous one. In a team-based setting, several actions occur simultaneously. Below is the full step-by-step breakdown, starting from the moment you identify a slow heart rate in a pediatric patient.
Bradycardia in a pediatric patient is defined as a heart rate below 60 beats per minute with signs of poor perfusion. A slow heart rate alone does not confirm a problem. Your first task is to determine whether the bradycardia is causing cardiopulmonary compromise.
Assess the patient for the following 5 signs of cardiopulmonary compromise:
If none of these signs are present, move to Step 2. If any of these signs are present, move directly to Step 3.
A child with bradycardia but no signs of cardiopulmonary compromise does not require immediate intervention. Your goal at this stage is to support the patient, identify the underlying cause, and monitor closely for any deterioration.
Take the following 4 actions:
Reassess the patient frequently because the condition of the child in this category can deteriorate quickly. If signs of cardiopulmonary compromise develop at any point, move immediately to Step 3. If the patient remains stable, continue monitoring and prepare for the ALS team handoff.
A child showing signs of cardiopulmonary compromise needs immediate intervention. Do not delay treatment to gather more information. The three actions in this step occur rapidly and, in a team-based setting, simultaneously.
Open and maintain the airway first while providing high-flow oxygen via a non-rebreather mask or bag-mask ventilation. Attach a cardiac monitor and pulse oximeter, then establish IV or IO access if it is not already in place. Because hypoxia is the most common cause of pediatric bradycardia, correcting oxygenation and ventilation alone may resolve the issue without further intervention. If the heart rate improves with these steps, reassess the patient’s status before moving to medications.
If airway support does not resolve the bradycardia, administer medications without delay. Epinephrine is the first-line drug for bradycardia caused by poor perfusion, given at an IV or IO dose of 0.01 mg/kg with a maximum single dose of 1 mg. Repeat this dose every 3 to 5 minutes as needed. Atropine is used for bradycardia caused by increased vagal tone or primary atrioventricular (AV) block, administered at an IV or IO dose of 0.02 mg/kg. This dose has a minimum of 0.1 mg and a maximum of 0.5 mg, and it may be repeated once.
Transcutaneous pacing is indicated when bradycardia is caused by a primary heart conduction problem that does not respond to oxygen or medications. Because it is not a first-line intervention, consider pacing only after attempting airway support and drug therapy. Apply pacing pads to the child’s chest and back, then set the rate above their intrinsic heart rate. Increase the output until you confirm electrical capture on the monitor and mechanical capture by feeling a pulse that matches the paced rhythm. Provide sedation and analgesia whenever possible, as this procedure is painful for a conscious patient.
If the child loses their pulse at any point during bradycardia management, the PALS Bradycardia Algorithm ends. Transition immediately to the PALS Cardiac Arrest Algorithm and begin chest compressions without delay. Place the patient on a firm, flat surface using the two-finger or two-thumb encircling technique for infants, or one or two hands for children depending on their size. Begin chest compressions at a rate of 100 to 120 per minute and to a depth of at least one-third the diameter of the chest.
Do not pause to reassess the bradycardia because pulseless arrest requires a separate sequence of interventions. This transition includes rhythm analysis, defibrillation if indicated, and advanced airway management. Recognizing this critical decision point immediately and acting without hesitation is essential for the best patient outcome.
Bradycardia in a child rarely develops without an underlying cause. Identifying that cause early guides your treatment decisions and improves outcomes. Pediatric bradycardia falls into two broad categories which are as follows:
Primary bradycardia originates from a structural or electrical problem within the heart itself. There are four common causes of primary bradycardia in children:
Primary bradycardia does not resolve with oxygenation alone. These patients often require medications, pacing, or specialist intervention.
Secondary bradycardia is far more common in children than primary bradycardia. It develops as a response to an external physiological stress rather than a cardiac problem. There are six common causes of secondary bradycardia in children:
Correcting oxygenation and ventilation is the first priority in secondary bradycardia. In many cases, restoring adequate oxygen delivery is enough to normalize the heart rate without any further intervention.
Three medications are used in the PALS Bradycardia Algorithm. Each one has a specific indication, dose, and route. Knowing when to use each one is as important as knowing the dose.
Pediatric and adult bradycardia share the same definition but require fundamentally different approaches. The underlying causes, drug doses, and intervention thresholds all differ based on age and physiology. The table below outlines the key differences.
The PALS Bradycardia Algorithm involves rapid clinical decisions, weight-based drug dosing, and age-specific interventions that cannot be mastered through reading alone. Pediatric emergencies are high-stakes and low-frequency events, meaning most healthcare providers encounter them rarely but must respond perfectly when they occur. Simulation-based training closes this gap.
Physicians, nurses, paramedics, and respiratory therapists in pediatric or emergency care must maintain AHA PALS certification, which remains valid for two years. Whether you are preparing for an initial certification or an upcoming renewal, CPR Lifeline offers AHA-authorized PALS courses with pediatric-specific simulations covering every algorithm, including bradycardia, tachycardia, and cardiac arrest.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
Epinephrine is the first-line drug for symptomatic pediatric bradycardia with poor perfusion. Administer 0.01 mg/kg IV or IO, up to a 1 mg maximum dose. Conversely, Atropine is reserved for bradycardia caused by increased vagal tone or primary AV block rather than poor perfusion.
Start CPR when the child's heart rate drops below 60 beats per minute with signs of poor perfusion that do not respond to airway support and oxygenation. If the pulse is lost at any point, transition immediately to the PALS Cardiac Arrest Algorithm and begin chest compressions without delay.
The minimum atropine dose in pediatric patients is 0.1 mg IV or IO, regardless of the child's weight. Doses below 0.1 mg can paradoxically worsen bradycardia by producing a paradoxical vagal response. The maximum single dose is 0.5 mg and may be repeated once.
Transcutaneous pacing is indicated when bradycardia persists despite adequate airway support, oxygenation, and two rounds of medication. It is used specifically for bradycardia caused by a primary cardiac conduction problem, such as complete AV block. It is not a first-line intervention and should not replace or delay airway management and drug therapy.
The reversible causes of pediatric bradycardia are organized under the Hs and Ts framework. The Hs include hypoxia, hypovolemia, hypothermia, hydrogen ion excess (acidosis), and electrolyte abnormalities. The Ts include tension pneumothorax, cardiac tamponade, toxins, and thrombosis. Hypoxia is the most common reversible cause in children and should be addressed first.
Use a length-based resuscitation tape, such as the Broselow tape, to estimate weight in kilograms. Place the tape alongside the child from head to heel and read the corresponding weight range. This weight is then used to calculate all drug doses and equipment sizes. Do not estimate weight from appearance alone, as visual estimation significantly increases the risk of dosing errors.
PALS certification is valid for two years. Given the complexity of pediatric resuscitation and the low frequency of pediatric emergencies in most clinical settings, skills refreshers between certification cycles are strongly recommended to maintain competency.
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!
