The Adult Basic Life Support (BLS) Algorithm is the evidence-based, step-by-step sequence that guides your immediate response when a person loses a pulse or stops breathing normally. Developed and regularly updated by the American Heart Association (AHA), it defines the exact order of actions you must take before advanced medical care arrives.
Every second without intervention lowers the patient’s chance of survival, and that is exactly where basic life support steps in to make the difference. It covers everything from confirming scene safety to delivering chest compressions and using an AED. Whether you are a healthcare provider or a trained first responder, knowing this algorithm and applying it without hesitation is what keeps a patient alive in those first critical minutes.

The adult BLS algorithm is a sequence of actions that applies to any unresponsive adult patient who is not breathing normally or has no detectable pulse. It covers three core actions, which include recognizing cardiac arrest, activating the emergency response system, and delivering high-quality CPR with early defibrillation.
Each step in this algorithm follows a specific order because sequence matters in resuscitation. Starting chest compressions before confirming unresponsiveness or delaying defibrillation to perform extra ventilations will directly reduce survival outcomes for the patient. With this algorithm, you will learn to perform high-quality CPR by understanding its key metrics and recognizing the common mistakes that can hinder resuscitation efforts.
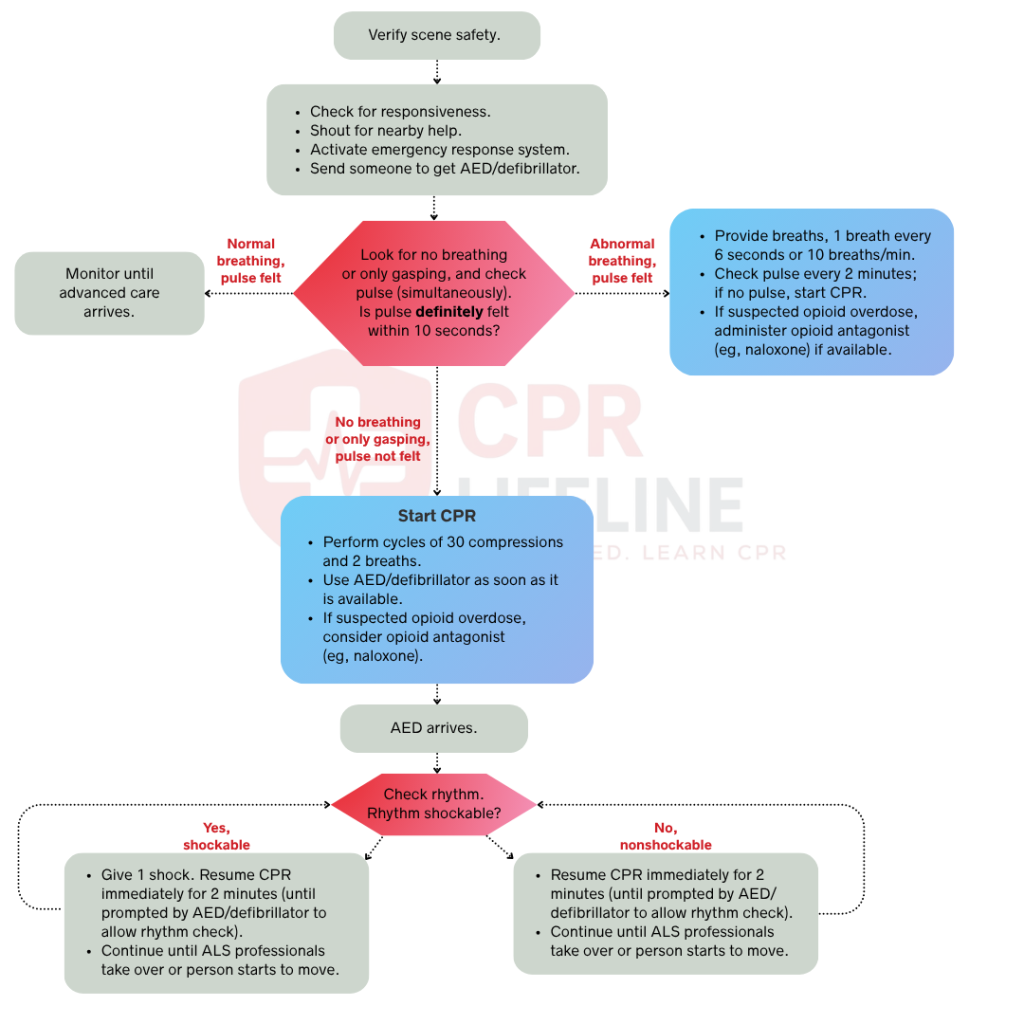
The Adult BLS Algorithm follows a linear sequence, but in multi-rescuer scenarios, several steps happen at once. Every action is time-sensitive and directly affects whether the patient survives. Below is the full step-by-step breakdown, starting from the moment you reach the patient.
Before you approach any unresponsive patient, you must confirm the scene is safe by scanning for hazards like traffic, electrical wires, or toxic substances. An injured responder cannot provide help, so you should only move the patient if staying in place creates an immediate danger. Always use personal protective equipment (PPE) when available, as maintaining scene safety is the essential foundation for every subsequent step in the resuscitation algorithm.
After confirming the scene is safe, kneel beside the patient and tap their shoulders firmly while shouting, “Are you okay?” to assess responsiveness. You must confirm they are unresponsive within a few seconds to avoid delaying the next steps.
Immediately call 911 or direct a specific bystander by pointing and saying, “You, call 911 now.” This specific assignment prevents the bystander effect and ensures a clear response while you simultaneously send another person to retrieve the nearest AED. If you are alone, you must call 911 yourself before continuing your assessment.
Once EMS is activated, you must assess the patient’s breathing and pulse at the same time by placing two fingers on the carotid artery. Simultaneously look at the chest for visible rise and fall, ensuring you complete this assessment in 10 seconds or less to avoid delaying the start of CPR.
There are three possible findings at this stage that determine your next steps.
A patient with a confirmed pulse and normal breathing does not need CPR. If they are unconscious but breathing, you must place them in the recovery position by rolling them onto their side and supporting the head to keep the airway clear. This position prevents obstruction from the tongue or secretions and reduces the risk of aspiration. Monitor the patient continuously and recheck their breathing and pulse every two minutes until EMS arrives. Stay alert for any change in responsiveness or skin color. If the patient loses their pulse or stops breathing, you must initiate CPR immediately.
Respiratory arrest occurs when a patient has a pulse but is not breathing normally. Your immediate goal is to deliver oxygen to prevent cardiac arrest. Open the airway by tilting the head back and lifting the chin, or use a jaw thrust if you suspect a spinal injury. Deliver one breath every 5 to 6 seconds, aiming for 10 to 12 breaths per minute. Each breath must last one second and produce a visible chest rise. Use a bag-mask device with a proper seal whenever it is available. Recheck the pulse every two minutes and initiate CPR immediately if the pulse is lost at any point.
No pulse indicates that the victim is in cardiac arrest, and you must begin chest compressions immediately. Place the heel of your dominant hand on the lower half of the sternum, place your other hand on top, interlace your fingers and keep your shoulders directly over your hands with straight arms.
Compress the chest at a rate of 100 to 120 compressions per minute and a depth of at least 2 to 2.4 inches. You must allow for full chest recoil and maintain a 30:2 compression-to-ventilation ratio, minimizing any interruptions to less than 10 seconds to ensure the most effective resuscitation.
As soon as the AED is available, turn it on and follow the audio prompts immediately. Attach the pads to the patient’s bare and dry chest. Place one pad below the right collarbone and the other on the left side below the armpit. You should only stop CPR while the device analyzes the rhythm or delivers a shock. The AED will classify the rhythm as either shockable or non-shockable. Each classification requires a different response.
Ventricular fibrillation and pulseless ventricular tachycardia are shockable rhythms that prevent the heart from pumping. Defibrillation is the definitive treatment for both. After the AED delivers a shock, resume CPR immediately for two minutes before the next rhythm check. Continue this cycle until the patient regains a pulse, advanced care arrives, or you are physically unable to continue. Every minute without defibrillation in a shockable rhythm reduces survival by 7 to 10 percent, so speed is critical at every step.
Asystole and pulseless electrical activity (PEA) do not respond to defibrillation, so the AED will not advise a shock. You must continue high-quality CPR without interruption and perform rhythm checks every two minutes. In a clinical setting, you should simultaneously investigate and treat reversible causes using the H’s and T’s framework, such as hypovolemia, hypoxia, or toxins. Continue CPR until a shockable rhythm develops, a pulse returns, or a qualified provider stops the resuscitation efforts.
High-quality CPR is the single most important factor in cardiac arrest survival. Performing the steps correctly is not enough because your performance directly determines whether blood reaches the brain and heart. Every provider must meet these specific standards to ensure the best possible outcome for the patient.
Maintain a compression rate of 100 to 120 per minute to maintain adequate circulation. Rates below 100 are too slow, while rates above 120 reduce depth and limit necessary chest recoil. You must compress to a depth of at least 2 inches but no more than 2.4 inches on an average adult. Compressions shallower than 2 inches fail to move blood effectively, while those deeper than 2.4 inches increase the risk of injury without improving outcomes. Use your body weight rather than arm strength to achieve consistent depth throughout the resuscitation.
Full chest recoil allows the chest to return completely to its natural position between compressions. Incomplete recoil keeps intrathoracic pressure elevated and reduces blood flow to the heart. You must avoid leaning on the chest and should slightly lift the heel of your hand between compressions without losing contact. Since fatigue is the primary cause of poor recoil, you should rotate the compressor role every two minutes when multiple rescuers are present to maintain quality.
Frequent or prolonged interruptions significantly reduce the overall effectiveness of CPR, so you must keep all pauses under 10 seconds. Acceptable reasons to pause compression include rhythm analysis, shock delivery, and airway placement. You should not pause for pulse checks outside of scheduled two-minute intervals.
Even trained providers make errors during cardiac arrest resuscitation. Most mistakes fall into predictable patterns. Recognizing them before you are in that situation is the best way to avoid them.
To achieve high-quality CPR, you must compress the chest between 2 and 2.4 inches using your body weight. Keep your arms straight and your shoulders directly over your hands. If the patient is on a soft surface, you should place a backboard underneath them or move them to the floor to ensure your compressions remain effective.
Deliver each breath over one second with just enough volume to produce a visible chest rise. You should avoid over-squeezing the bag to prevent excessive ventilation. Once an advanced airway is in place, you must limit ventilations to 10 breaths per minute and ensure you do not exceed that rate.
Send someone for the AED as soon as you confirm cardiac arrest. You must apply the pads without stopping chest compressions and only pause when the device is ready to analyze. Treat the AED setup as a task parallel to CPR and resume compressions within five seconds of any shock delivery.
Learning the Adult BLS Algorithm starts with understanding the steps, but performing them under pressure requires hands-on practice. While reading builds familiarity, a formal BLS certification course provides the structured, skills-based environment needed to convert that knowledge into life-saving action.
The American Heart Association provides BLS certification valid for two years, but critical skills like compression depth and AED use degrade without regular practice. You should not wait until your certification expires to refresh your knowledge. If you are ready to get certified or recertify, CPR Lifeline offers AHA-authorized BLS courses featuring a blended learning format and hands-on skills simulation. It is the most effective way to build the confidence and muscle memory this algorithm demands.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
Deliver compressions at a rate of 100 to 120 per minute and to a depth of at least 2 inches but no more than 2.4 inches. Use your body weight to achieve consistent depth and allow full chest recoil between each compression.
Each rescue breath should last one second and produce a visible chest rise. Do not force volume into the lungs. Over-ventilation raises intrathoracic pressure and reduces cardiac output during CPR.
Stop CPR only if the patient regains a pulse and begins breathing normally, a qualified provider assumes care and directs you to stop, or you are physically unable to continue further.
BLS certification is valid for two years. Renew your certifications before it expires. Compression depth, recoil quality, and AED proficiency all decline without regular practice, so periodic skills refreshers between certification cycles are strongly recommended.
BLS is the first tier of emergency cardiac care. It covers the immediate actions any trained responder takes, including chest compressions, rescue breathing, and AED use. ACLS builds on BLS and is designed for healthcare providers in clinical settings. It includes cardiac rhythm interpretation, intravenous medication administration, advanced airway management, and team-based resuscitation protocols.
For drowning victims, begin with 5 rescue breaths before starting standard CPR. Drowning arrest is hypoxia-driven, so oxygen comes first. For opioid overdose victims, administer naloxone if available and deliver rescue breathing if a pulse is present. Start CPR only if the pulse is lost.

Home | About Us | Classes | Locations | Blogs | FAQ’s | Group Training | Contact Us
Copyright © 2025 cprlifeline. All Rights Reserved. Powered by Splendour Group
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!