Achieving Return of Spontaneous Circulation (ROSC) is a critical milestone, but it marks the beginning of recovery rather than the end of resuscitation. The heart is beating again, but the fight for survival and neurological recovery continues. Post-cardiac arrest care is the systematic management of patients immediately after ROSC. This phase focuses on three goals, which are stabilizing circulation, protecting the brain, and identifying the cause of arrest.
The ACLS Post-Cardiac Arrest Care Algorithm provides a structured framework for this transition from active resuscitation to patient stabilization. It guides you through hemodynamic support decisions, coronary reperfusion timing, and neuroprotection strategies. You will learn specific blood pressure targets that maintain brain perfusion, understand why hyperventilation harms neurological outcomes, and identify which patients need immediate coronary angiography.

The ACLS Post-Cardiac Arrest Care Algorithm provides a systematic framework for stabilizing vital systems after the heart restarts. It covers step-by-step decision points for airway management, oxygenation targets, blood pressure control, and coronary reperfusion. The AHA designed this protocol to standardize care during the critical window when your interventions have the greatest impact. This algorithm integrates with other ACLS protocols to create a comprehensive approach to cardiac arrest management.
The main goal of this algorithm is to optimize survival with a favorable neurological function. You use this protocol to address Post-cardiac arrest syndrome (PCAS), a condition that includes four components, which are brain injury, myocardial dysfunction, systemic ischemia-reperfusion response, and the persistent precipitating pathology.
The post-cardiac arrest algorithm provides a structured framework to stabilize patients after ROSC, focusing on respiratory optimization, hemodynamic support, and neuroprotective strategies to improve long-term survival.
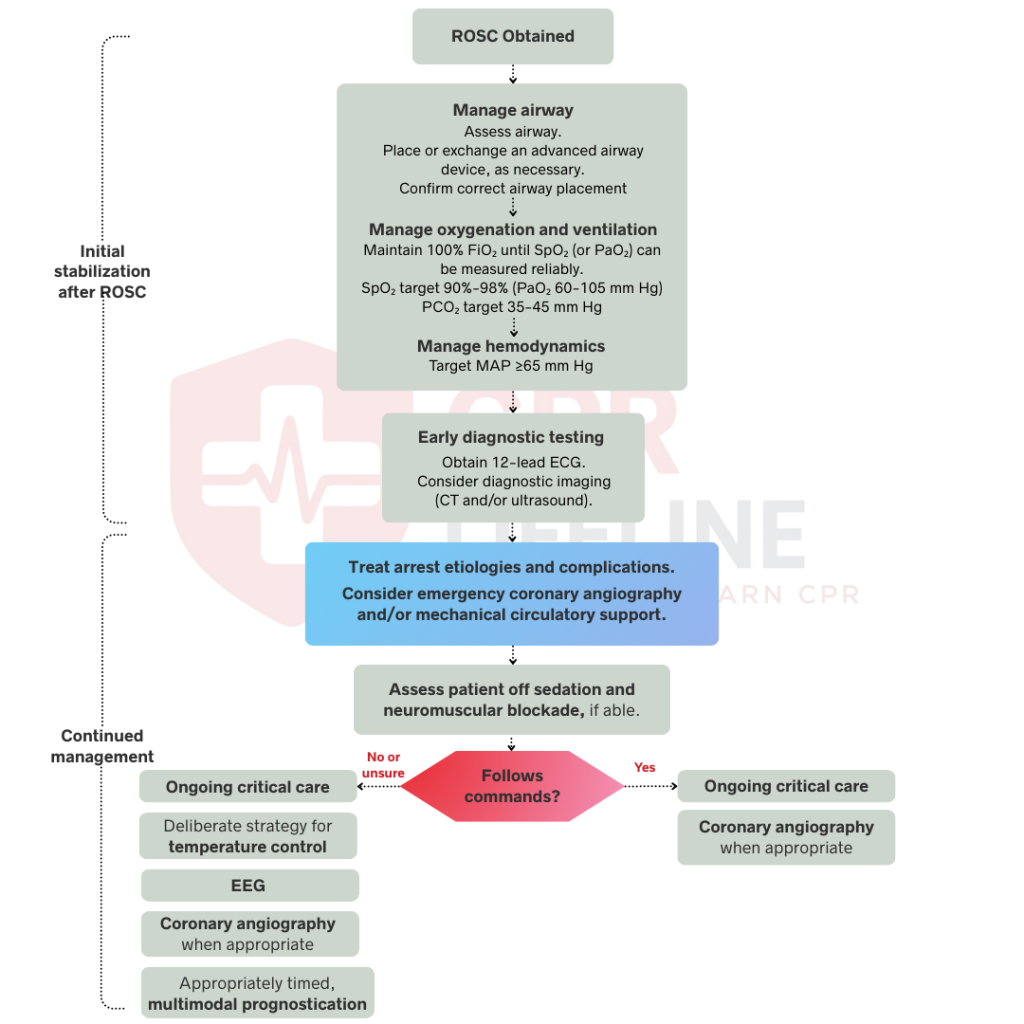
The initial stabilization phase begins immediately after ROSC and focuses on three critical priorities, which are airway management, respiratory optimization, and hemodynamic stabilization. These interventions occur concurrently when possible, but follow this prioritized sequence when you must address them individually.
Manage the airway immediately after achieving ROSC by ensuring adequate ventilation and oxygenation. Consider early placement of an endotracheal tube for patients who cannot protect their airway or remain unresponsive. Use waveform capnography or capnometry to confirm proper endotracheal tube placement immediately after intubation. Continue monitoring with continuous waveform capnography throughout post-arrest care. Waveform capnography detects tube dislodgement, provides ventilation feedback, and monitors cardiac output through ETCO₂ values. Secure the tube and verify position with chest X-ray once the patient stabilizes.
Start ventilation at 10 breaths per minute to avoid hyperventilation that causes cerebral vasoconstriction. Titrate FiO₂ to maintain SpO₂ between 90-98% and avoid both hyperoxia and hypoxia. Target PaCO₂ between 35-45 mmHg by adjusting ventilation rate and tidal volume. Monitor end-tidal CO₂ continuously to ensure adequate ventilation. Obtain arterial blood gas measurements to confirm oxygenation and ventilation targets are met. Excessive ventilation reduces cerebral blood flow and worsens neurological outcomes, while hypoxia causes additional brain injury.
Maintain systolic blood pressure above 90 mmHg or mean arterial pressure above 65 mmHg to ensure adequate organ perfusion. Administer crystalloid fluid boluses for volume resuscitation in hypotensive patients. Give vasopressor support if hypotension persists after adequate fluid administration. Norepinephrine serves as the first-line vasopressor starting at 0.1 mcg/kg/min. Add inotropic support with dobutamine if cardiac output remains inadequate despite acceptable blood pressure. Place an arterial line for continuous blood pressure monitoring to detect hypotension immediately.
Obtain a 12-lead ECG as soon as possible after ROSC to identify ST-elevation myocardial infarction requiring emergency cardiac intervention. Interpret the ECG for ST-segment elevations, new bundle branch blocks, and other acute changes. Compare with previous ECGs when available because cardiac arrest itself can cause transient ECG abnormalities. STEMI presentation requires immediate activation of the cardiac catheterization lab regardless of the patient’s mental status. Early coronary angiography and percutaneous intervention improve survival in post-arrest STEMI patients.
After initial stabilization, your focus should shift to targeted interventions based on neurological status. These evaluations occur concurrently so that targeted temperature management and cardiac interventions receive equal priority in your management plan.
Assess whether your patient follows commands to determine the appropriate management pathway. Patients who follow commands are considered awake and should receive standard critical care management without targeted temperature management. Comatose patients who do not follow commands require targeted temperature management and additional neuroprotective interventions. Perform this assessment after initial stabilization is complete. Use simple commands like “squeeze my hand” or “open your eyes” to evaluate responsiveness. Document the Glasgow Coma Scale score to establish baseline neurological status.
Comatose patients who cannot follow commands after ROSC require intensive neuroprotective interventions. Start targeted temperature management immediately, targeting 32-36°C for 24 hours using cooling devices with feedback loops. Initiate cooling with 30 mL/kg of 4°C intravenous saline. Obtain a brain CT to evaluate for hemorrhage and structural abnormalities. Provide continuous EEG monitoring for at least 24 hours to detect non-convulsive seizures occurring in 20-30% of survivors. Continuously monitor core temperature using esophageal, bladder, or rectal probes. Maintain normoxia (SpO₂ 92-98%), normocapnia (PaCO₂ 35-45 mmHg), and euglycemia (glucose 140-180 mg/dL). Provide lung-protective ventilation with tidal volumes of 6-8 mL/kg ideal body weight.
Patients who follow commands after ROSC should receive standard critical care management without targeted temperature management. Maintain adequate oxygenation with SpO₂ between 92-98% and ventilation with PaCO₂ between 35-45 mmHg. Monitor hemodynamic stability and maintain blood pressure above target thresholds. Monitor neurological status closely for any deterioration that would require escalation of interventions. Identify and treat underlying causes that precipitated the cardiac arrest through systematic evaluation. Consider cardiac catheterization for patients with suspected acute coronary syndrome based on ECG findings and clinical presentation. Transfer to the appropriate level of care based on patient needs and available facility resources.
To prevent recurrent arrest and optimize survival, begin a systematic evaluation for reversible causes using the Hs and Ts framework. This assessment should be supported by immediate laboratory tests such as electrolytes, arterial blood gas, lactate, and troponin. Consider performing a bedside ultrasound and chest X-ray to identify pneumothorax and pericardial effusion. When pulmonary embolism or another emergent condition is suspected, prioritize CT imaging. Treat identified causes immediately with fluid resuscitation, electrolyte correction, needle decompression, pericardiocentesis, antidotes for toxins, or emergency cardiac catheterization to prevent recurrent arrest and improve the survival outcome of the patient.
Begin prognostication no earlier than 72 hours after ROSC, once TTM is complete and any sedation has fully cleared. This assessment must be multimodal, weaving together several key findings to build a complete clinical picture, including absent pupillary and corneal reflexes on examination, a bilateral absence of the N20 SSEP cortical wave, malignant EEG patterns, and evidence of gray-white matter loss on CT or diffusion restriction on MRI. No single finding on its own is sufficient to determine a poor prognosis. When assessment indicates poor prognosis, involve palliative care, communicate findings clearly to the family, and honor what the patient wishes.
Engage expert consultation from cardiology, intensive care, and neurology to guide comprehensive post-cardiac arrest management. A coordinated, multidisciplinary team approach improves outcomes by ensuring adherence to established protocols and delivering specialized care.
If your facility lacks the necessary resources, consider a timely transfer to a specialized cardiac arrest center. These centers provide 24/7 cardiac catheterization, expertise in targeted temperature management, continuous EEG monitoring, and dedicated post-arrest care teams. Continue systematic, evidence-based management throughout the patient’s hospitalization to optimize recovery.
The H’s and T’s mnemonic identifies ten reversible causes of cardiac arrest that require immediate recognition and treatment. Evaluating each cause during post-ROSC care prevents recurrent arrest and improves survival by addressing underlying conditions that triggered the initial event.
The difference between neurologic recovery and severe brain damage happens in the critical hours after ROSC. Mastering this algorithm means you can systematically optimize oxygenation, stabilize hemodynamics, implement targeted temperature management, and protect your patient’s brain from secondary injury. Every step you execute correctly increases your patient’s chance of walking out of the hospital with meaningful function.
Maintaining current ACLS certification ensures you stay updated with the latest evidence-based guidelines and can execute these protocols confidently during actual emergencies. At CPR Lifeline, you can find comprehensive ACLS training programs that fit your schedule and learning preferences. We provide blended learning formats that combine online coursework with hands-on practice sessions, allowing you to learn at your own pace while still gaining essential practical skills.
Our ACLS certification course covers the complete post-cardiac arrest care algorithm with real-world scenarios and expert instruction. Join us and learn the skills that turn resuscitation into recovery.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
The ACLS post-cardiac arrest care algorithm is a systematic protocol for managing patients after achieving return of spontaneous circulation (ROSC). It optimizes oxygenation, ventilation, hemodynamics, and neuroprotection to maximize survival with favourable neurological outcomes.
Emergency cardiac catheterization should be performed immediately for post-arrest patients with ST-elevation on ECG, indicating acute myocardial infarction. For patients without clear STEMI, consider catheterization based on suspected cardiac etiology, hemodynamic instability, and clinical judgment.
Wait at least 72 hours after cardiac arrest, and longer if therapeutic hypothermia was used, before making a neurological prognosis. Use a multimodal approach, including clinical exam, EEG, imaging, and biomarkers, rather than relying on single predictors for accurate assessment.
Initiate TTM as soon as possible after achieving ROSC in any comatose patient who does not follow commands. Early initiation is associated with faster achievement of target temperature and potentially better neurological outcomes.
Post-cardiac arrest syndrome (PCAS) includes four components which includes, anoxic brain injury, myocardial dysfunction, systemic ischemia-reperfusion response, and the persistent precipitating pathology. This syndrome explains why patients remain critically ill even after successful resuscitation and require intensive targeted interventions.
You can prevent re-arrest by optimizing oxygenation and ventilation, maintaining adequate blood pressure, correcting electrolyte imbalances, treating underlying causes, and monitoring continuously. Avoid hyperventilation, ensure appropriate sedation, and address reversible conditions like ischemia, acidosis, or arrhythmias promptly.
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!
