
The ACLS Bradycardia with a Pulse Algorithm is far more than a simple protocol because it represents a structured way of thinking built on decades of AHA evidence-based research. When a patient’s heart rate drops below 50 beats per minute and their body begins to show signs of compromise, you do not have the time to second-guess your next move.
This algorithm prioritizes a clear sequence of interventions by helping you recognize what symptomatic bradycardia means, the step-by-step treatment protocol, and medication dosages. By following these steps, you can more effectively determine whether a patient requires immediate intervention or if you have the time to monitor their condition more closely while addressing the root of their slow heart rate.

The ACLS bradycardia algorithm is a systematic protocol designed to help healthcare professionals manage patients with slow heart rates, typically below 50 beats per minute. The algorithm guides clinicians through patient assessment, helps identify when medications are necessary, and determines whether advanced interventions like temporary pacing are required to stabilize the patient.
One of the most important things to understand about this algorithm is that it applies exclusively to patients who have a detectable pulse. If no pulse is present, the provider must immediately transition to the cardiac arrest algorithm, as the clinical priorities shift entirely. Making this distinction is very important because following the wrong protocol for a pulseless patient can cost critical time that they don’t have.
The ACLS approach focuses on recognizing true cardiopulmonary compromise, as a slow heart rate only becomes clinically significant when it leads to inadequate systemic perfusion. Rather than treating the number on the monitor alone, you must evaluate the patient for these specific signs that indicate their body is no longer compensating.
If the patient shows one or more of these findings, you must begin the ACLS bradycardia algorithm without delay.
The ACLS Bradycardia with a Pulse Algorithm provides a structured escalation pathway. To ensure the best possible outcomes, rescuers must follow a clear, simple sequence that focuses on early action and minimal delay in escalation.
Start with the fundamentals of emergency cardiovascular care. Your first actions create the foundation for everything that follows.
This step runs parallel to everything else and is not a one-time check. While you assess and treat the bradycardia, always search for reversible causes.
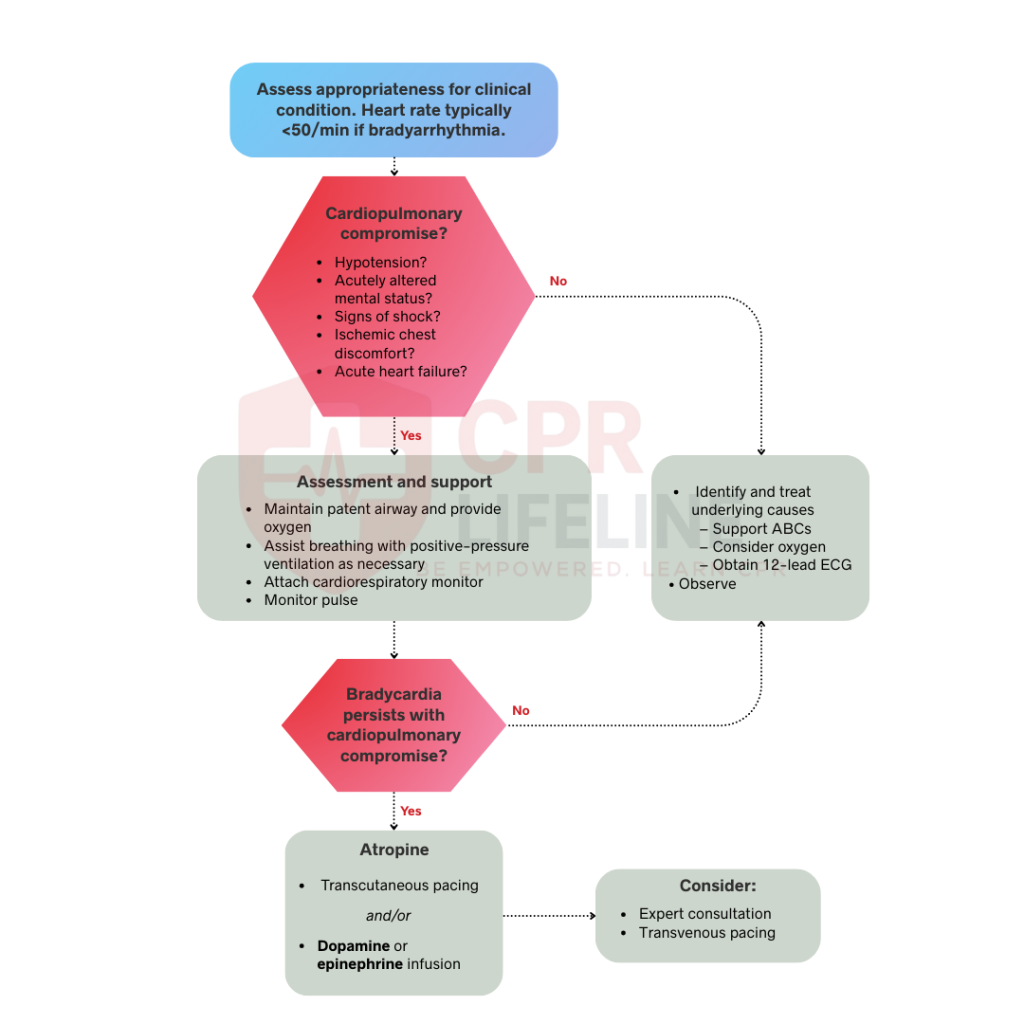
Before escalating care, confirm if the patient is clinically stable or not. A heart rate typically needs to be less than 50 beats per minute for bradyarrhythmia to be the primary cause of distress.
Determine if cardiopulmonary compromise still exists. Ask these key questions:
If the patient’s answer to all of these is NO, monitor and observe the patient. Continue to identify and treat underlying causes, but do not give emergency medications or start pacing. If the answer to any is YES, proceed immediately to emergency treatment.
For patients with cardiopulmonary compromise from bradycardia, atropine is the first-line medication. It blocks vagal effects on the heart and typically increases heart rate within minutes.
Atropine is often ineffective for high-risk heart blocks because they involve structural issues below the AV node. Do not give atropine to hypothermic patients because it can cause ventricular fibrillation. Warm the patient first before attempting pharmacologic treatment. If you’ve given 3 mg total without adequate response, atropine has failed and you need to move to other interventions and escalate treatment.
If the maximum dose of Atropine fails or the patient is severely unstable, you must choose from three secondary interventions based on your available resources:
Both vasopressor infusions take time to prepare and require careful monitoring. They are best used when a patient responds to atropine but needs ongoing support, or when transcutaneous pacing is not immediately available.
If bradycardia persists despite the above interventions, the patient likely needs definitive treatment with a permanent or temporary transvenous pacemaker. Contact cardiology immediately for transvenous pacing, where a wire is threaded through a central vein directly into the right ventricle. This provides more reliable pacing than transcutaneous pacing and causes no discomfort.
Patients with Mobitz Type II or Third-Degree heart block almost always require transvenous pacing, as these rhythms carry an extremely high risk of progressing to complete heart block and cardiac arrest.
When bradycardia doesn’t respond as expected, a reversible underlying cause is almost always to blame. The H’s and T’s give you a systematic way to identify it and address it quickly.
Understanding the ACLS Bradycardia Algorithm is what prepares you to navigate emergencies without any hesitation. Knowing how to identify symptoms quickly, start with the right treatment, and escalate care when needed can directly improve patient outcomes.
The ACLS Bradycardia algorithm focuses on three key steps, which include recognizing symptomatic bradycardia, starting treatment with atropine, and moving to pacing or medication infusions if the patient doesn’t respond. This structured approach follows current ACLS guidelines and helps you provide safe, effective emergency care.
If you’re ready to strengthen your emergency response skills and master advanced cardiac care protocols, we encourage you to enroll in an ACLS course with us. Join the thousands of healthcare professionals who trust CPR Lifeline for their certification needs.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
In ACLS, bradycardia is officially a heart rate under 60 beats per minute. However, we usually don't get aggressive with treatment unless the rate drops below 50 and the patient starts showing signs of poor perfusion.
Atropine is your go-to first-line drug. We give a 1 mg IV bolus right away. It’s effective because it blocks the vagus nerve, allowing the heart to speed back up to a safer rhythm.
Not necessarily. While it's great for sinus bradycardia, it often fails in high-grade blocks like Mobitz II or Third-Degree. In those cases, the electrical issue is too deep for Atropine to fix, so we move to pacing.
The maximum dose for atropine is 3 mg total. We give 1 mg every three to five minutes. Once you hit that 3 mg limit, the receptors are fully occupied. If it hasn't worked by then, you must switch to other interventions.
Avoid it in hypothermic patients, as it can trigger V-fib. It’s also ineffective for heart transplant patients because their vagus nerve is severed. Lastly, don't waste time on it if your patient has a high-risk heart block.
The ACLS bradycardia algorithm does not apply to cardiac arrest situations (treat with the pulseless electrical activity algorithm) or to asymptomatic patients who do not need emergency intervention.

Home | About Us | Classes | Locations | Blogs | ACLs – Algorithm | FAQ’s | Group Training | Contact Us
Copyright © 2025 cprlifeline. All Rights Reserved.
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!