The acute coronary syndrome algorithm is a structured clinical framework designed to manage one of the most time-critical emergencies in medicine. Acute coronary syndrome refers to a series of life-threatening cardiac conditions caused by sudden reduced blood flow to the heart, encompassing STEMI, NSTEMI, and unstable angina. Without this algorithm, the risk of misclassification and delayed reperfusion increases significantly, costing approximately 2 million cardiomyocytes for every minute of delayed treatment.
The 2025 AHA Acute Coronary Syndrome Algorithm gives you a clear, step-by-step framework to move from initial chest pain recognition through ECG interpretation, risk stratification, reperfusion decisions, and post-stabilization care.

The acute coronary syndrome algorithm is a structured set of guidelines that guides you through the diagnosis, risk stratification, and treatment of suspected cardiac ischemia. It translates complex, time-sensitive data into clear decision points, ensuring that every action from initial presentation to definitive treatment follows a logical, evidence-based sequence.
The primary purpose of this protocol is to eliminate guessworks under high-pressure clinical situations. By anchoring every decision to objective findings like 12-lead ECG results, serial troponin levels, and validated risk scores, the algorithm ensures you apply the correct intervention at the precise time required. This systematic approach allows you to determine with confidence whether a patient requires immediate reperfusion or a specialized hospital treatment plan.
The ACS algorithm functions as a sequential clinical roadmap where each decision point determines the next stage of intervention. This progression ensures that from the moment of first contact, your diagnostic findings directly trigger the appropriate reperfusion or medical management strategy.
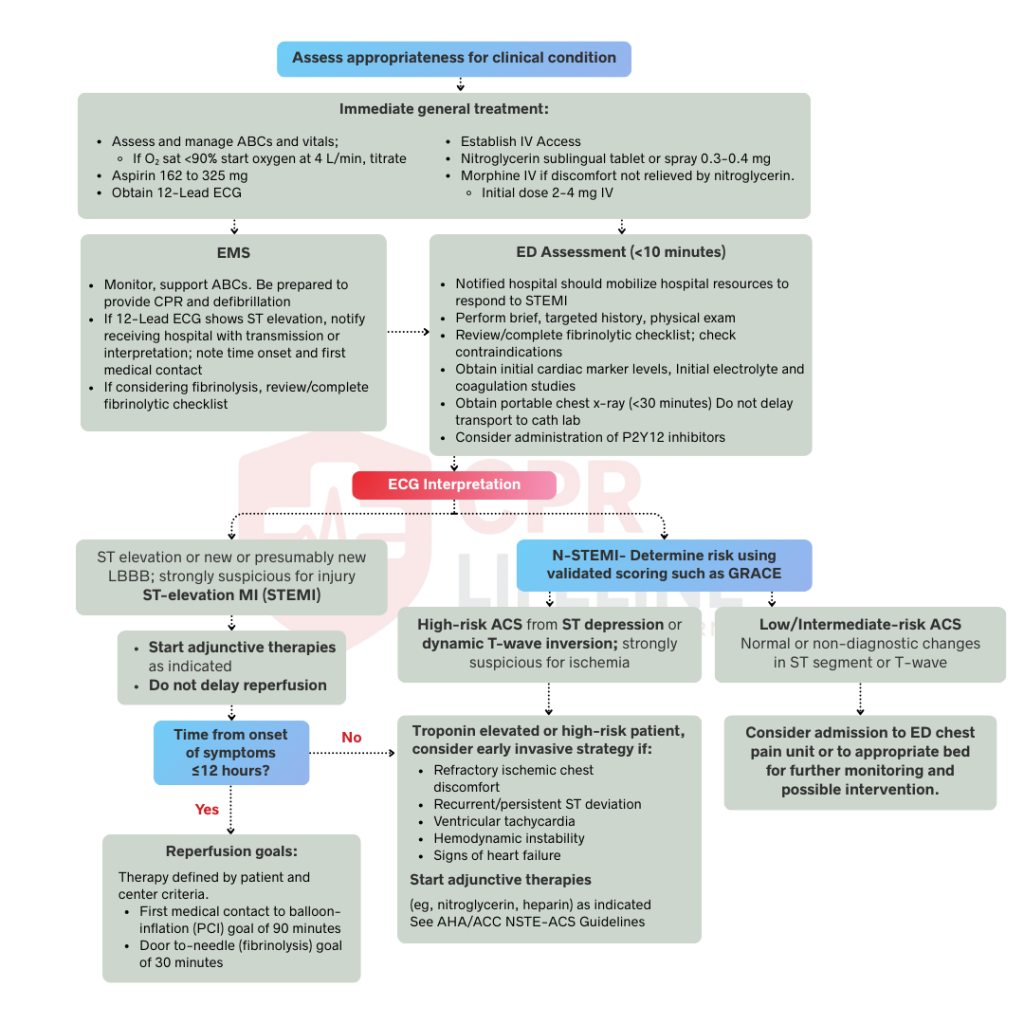
Your primary objective is rapid recognition, as typical ACS symptoms like chest pain, jaw or arm radiation, diaphoresis, and shortness of breath require an immediate clinical response. Within the first 10 minutes, you must establish IV access, start continuous cardiac monitoring, and ensure the patient chews 162–325 mg of aspirin for faster buccal absorption. Reserve supplemental oxygen only for those whose SpO₂ drops below 90% to avoid unnecessary hyperoxia.
In this phase you follow a precise sequence by interpreting the 12-lead ECG, confirming the diagnosis using serial troponins, and then apply a risk-scoring system to determine the urgency of intervention. This systematic method minimizes delays and helps align the medical team on the necessary treatment path.
You must obtain a 12-lead ECG within 10 minutes of arrival, as the findings dictate your entire clinical pathway. A STEMI is diagnosed by ST elevation of ≥1mm in two contiguous limb leads or ≥2mm in precordial leads. For NSTEMI or unstable angina, look for ST depression or T-wave inversions alongside ischemic symptoms. If the patient is inferior STEMI positive, always obtain right-sided leads (V4R) to screen for RV infarction, which requires avoiding nitrates in favor of IV fluids.
If the ECG does not show STEMI, confirm the diagnosis with serial troponins. High-sensitivity troponin (hs-cTnI or hs-cTnT) allows faster rule-in and rule-out compared to conventional troponin. Distinguish NSTEMI from Unstable Angina by identifying elevated troponin levels alongside ischemic symptoms or ECG changes, though high-sensitivity assays have made true cases of Unstable Angina increasingly rare in modern clinical practice.
Finally, use the GRACE score to determine how urgently you need to act. The GRACE score is considered more accurate for predicting in-hospital and 6-month mortality. It uses eight variables which include, age, heart rate, systolic blood pressure, serum creatinine, Killip class, cardiac arrest at presentation, ST deviation on ECG, and troponin elevation. A GRACE score above 140, significant troponin elevation, or dynamic ECG changes indicates an early invasive strategy within 24 hours, while clinical features such as hemodynamic instability, refractory ischemia, or life-threatening arrhythmias require immediate intervention within 2 hours regardless of the score.
The treatment pathway at this stage is determined entirely by your diagnostic findings, directing STEMI patients into immediate reperfusion while NSTEMI and high-risk ACS patients follow a strategy of antiplatelet therapy, anticoagulation, and timed invasive intervention.
In STEMI management, you are required to hit key targets including a door-to-balloon time of 90 minutes or less, a door-to-needle time for fibrinolysis within 30 minutes, or first medical contact-to-balloon within 120 minutes. Primary PCI is the preferred reperfusion strategy for complete revascularization, but if unavailable within the 120-minute window, you must administer weight-based fibrinolytics like Tenecteplase, Alteplase, or Reteplase. Ensure that no absolute contraindications exist, such as prior intracranial hemorrhage, active bleeding, or recent ischemic stroke. After fibrinolysis, transfer the patient to a PCI-capable center for angiography within 3 to 24 hours.
In NSTEMI and high-risk ACS, initiate aspirin immediately for all patients without contraindications and add a P2Y12 inhibitor (Ticagrelor or Prasugrel) according to your institutional protocol and cardiology guidance. For anticoagulation, utilize unfractionated heparin when an early invasive strategy is planned, enoxaparin as an alternative, or fondaparinux for conservative strategies to minimize bleeding risk. You must choose an invasive strategy based on risk levels, with immediate intervention required within 2 hours for refractory ischemia or hemodynamic instability and an early 24-hour strategy for patients with a GRACE score above 140 or significant troponin elevations.
Understanding the medications used in the ACS algorithm is essential for executing each phase of management with precision. Each drug targets a specific mechanism in the ischemic process, and correct dosing and timing are as critical as the decision to use them.
Prior to discharge, continue telemetry monitoring based on risk levels and obtain an echocardiogram to assess the left ventricular ejection fraction, as this measurement dictates your long-term medical strategy. You must build a comprehensive discharge plan including high-intensity statins to hit strict LDL targets and 12 months of dual antiplatelet therapy, though this period may be shortened for patients with high bleeding risk. For those with an ejection fraction of 40% or below, or those with multiple health issues like diabetes and hypertension, initiate an ACE inhibitor or ARB and continue beta-blockers for at least a year. Finally, add an aldosterone antagonist if the ejection fraction is 35% or below with heart failure symptoms, and ensure every patient is referred to cardiac rehabilitation to reduce their risk of cardiovascular mortality by roughly 25%.
The acute coronary syndrome algorithm serves as a high-velocity clinical framework designed to minimize decision time when every minute is critical for myocardial survival. This branching pathway demands rapid ECG interpretation, precise troponin-based diagnosis, and validated risk stratification to ensure guideline-directed therapy is timed perfectly to each patient’s specific risk level. By standardizing these essential steps, the algorithm transforms complex diagnostic data into a clear roadmap for immediate action.
Confident application of this algorithm requires more than just reading about it but rather hands-on training that reinforces critical decision points under pressure. At CPR Lifeline, we offer a flexible ACLS certification course through a blended learning format, allowing you to complete online modules on your schedule before finishing your skills check in person.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
The ACS algorithm is a systematic clinical framework that directs the diagnosis and management of STEMI, NSTEMI, and unstable angina. It streamlines your decision-making by anchoring every action to 12-lead ECG findings, serial troponin results, and validated risk stratification scores.
The three types include STEMI, NSTEMI, and unstable angina, all of which involve acutely reduced or obstructed blood flow to the myocardium. While STEMI is the most time-critical due to complete occlusion, all three require rapid intervention to prevent further cardiac damage.
Aspirin is your first-line intervention, with 162 to 325 mg administered and chewed immediately to inhibit platelet aggregation. This is typically followed by a P2Y12 inhibitor such as Ticagrelor or Prasugrel once the clinical strategy is established.
Diagnosis relies on a triad of tools which are a 12-lead ECG obtained within 10 minutes of arrival, high-sensitivity troponin levels measured at presentation and repeated at 1–2 hours, and a validated risk score like GRACE to determine the probability of a major event.
STEMI demands immediate reperfusion with a door-to-balloon target of 90 minutes, whereas NSTEMI management is risk-guided. For NSTEMI, catheterization timing can range from an immediate 2-hour window for unstable patients to a 72-hour window for those at intermediate risk.
You should initiate fibrinolysis when primary PCI cannot be performed within 120 minutes of first medical contact. Aim for a door-to-needle time of 30 minutes and ensure the patient is transferred to a PCI-capable center within 3 to 24 hours for follow-up intervention.
High-sensitivity troponin detects myocardial injury much earlier and at lower concentrations than older assays. This precision allows for rapid rule-in or rule-out decisions within 1 to 2 hours, significantly reducing ED overcrowding and delays in definitive care.
Standard DAPT duration is 12 months following the placement of a drug-eluting stent. However, you should shorten this to 3 to 6 months for patients at high bleeding risk or consider extending it beyond a year for those with high ischemic risk and low bleeding complications.
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!
