
Achieving return of spontaneous circulation is not the end of resuscitation. It is the beginning of the next critical phase. Children who survive cardiac arrest remain at high risk of secondary organ injury, hemodynamic instability, and neurological deterioration in the hours that follow. The PALS Post-Resuscitation Care Algorithm gives you a structured, evidence-based sequence to stabilize the patient, protect the brain, and transition to definitive care after ROSC is confirmed.
The quality of post-resuscitation care directly determines whether a child survives with a favorable neurological outcome. Poorly managed oxygenation, blood pressure, temperature, and glucose in the post-arrest period can undo the gains made during resuscitation. This algorithm guides you through each intervention in the correct order, so your response is systematic from the moment the pulse returns.

The PALS Post-Resuscitation Care Algorithm is the AHA-developed protocol for managing pediatric patients immediately after return of spontaneous circulation following cardiac arrest. It applies to any child who achieves ROSC after resuscitation, regardless of the initial arrest rhythm or underlying cause. The algorithm covers airway and ventilation management, oxygenation targets, hemodynamic support, temperature management, glucose control, and neurological monitoring.
The algorithm is designed to address post-cardiac arrest syndrome, a condition that develops after resuscitation and involves widespread organ dysfunction caused by ischemia-reperfusion injury. In children, the brain and cardiovascular system are the most vulnerable organs during this period. Every intervention in this algorithm is targeted at preventing secondary injury to these systems while the underlying cause of arrest is identified and treated.
Post-resuscitation care is not a single intervention. It is a coordinated sequence of time-sensitive actions that occur simultaneously in a team-based setting. Each step in the PALS Post-Resuscitation Care Algorithm targets a specific physiological system at risk of secondary injury after ROSC. Below is the full step-by-step breakdown, starting from the moment the return of spontaneous circulation is confirmed.
Secure and maintain the airway immediately after ROSC. Any child who cannot protect their own airway requires endotracheal intubation. Once the airway is secured, you should target a tidal volume of 6 to 8 mL/kg at an age-appropriate respiratory rate while avoiding hyperventilation to maintain a PaCO2 of 35 to 45 mmHg. Hypocapnia causes cerebral vasoconstriction and reduces cerebral blood flow. Use continuous waveform capnography to monitor end-tidal CO2 and guide ventilation adjustments in real time.
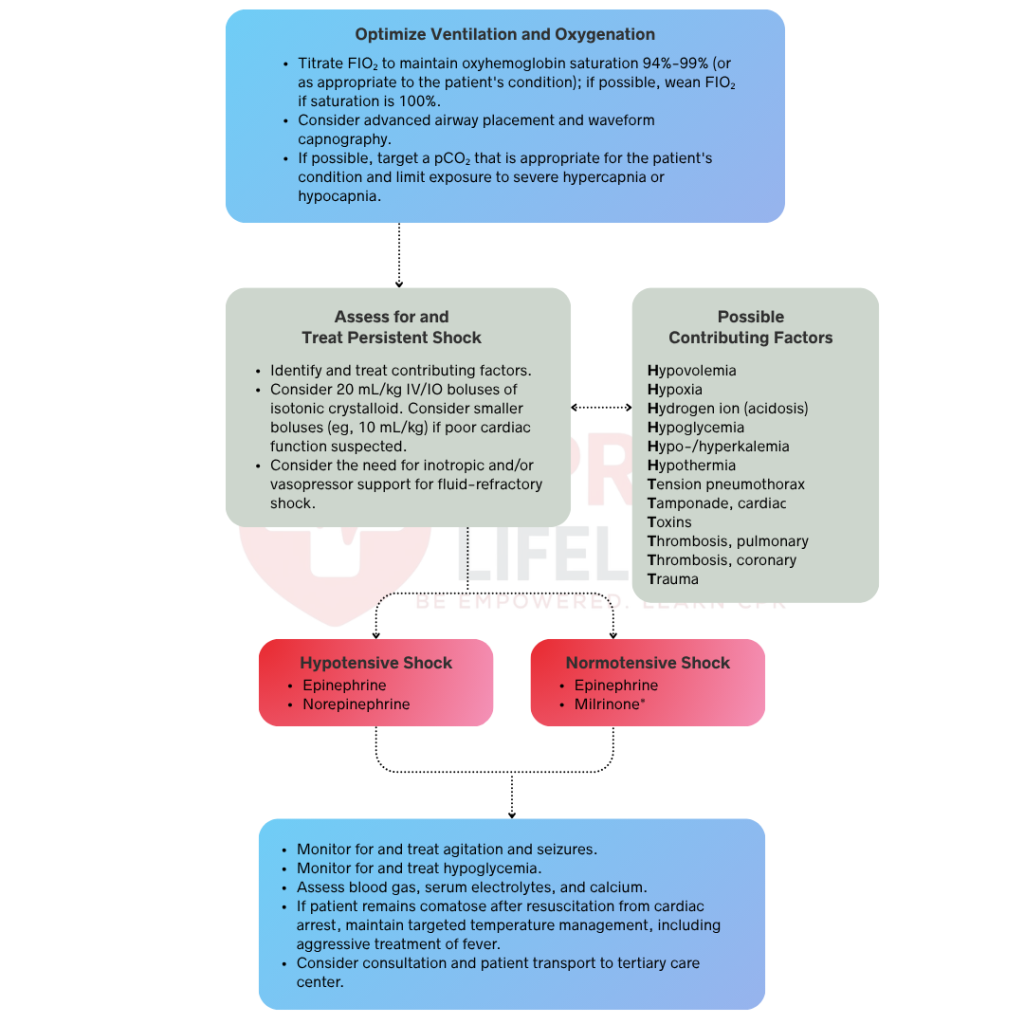
Once the airway is secured, you should titrate oxygen to maintain SpO2 between 94 and 99 percent because hyperoxia causes oxidative stress and worsens reperfusion injury to the brain and myocardium. Reduce the fraction of inspired oxygen (FiO2) as soon as the patient is stable enough to tolerate it while maintaining the target SpO2 range. If arterial blood gas monitoring is available, you should target a PaO2 of 60 to 300 mmHg while taking care to avoid hypoxia at all times. Any SpO2 reading below 94 percent requires an immediate reassessment of the airway, ventilation, and oxygen delivery.
Hypotension after ROSC reduces oxygen delivery to the brain and vital organs and must be corrected immediately. If hypotension is present, administer an isotonic crystalloid bolus of 10 to 20 mL/kg IV or IO and reassess perfusion after each bolus. If hypotension persists despite fluid resuscitation, you should initiate vasoactive therapy with epinephrine or dopamine as continuous IV or IO infusions titrated to effect. Target a mean arterial pressure at or above the fifth percentile for age. You must also correct metabolic abnormalities, including acidosis and electrolyte imbalances, because these issues directly impair myocardial function during the post-arrest period.
Fever worsens neurological outcomes after cardiac arrest and must be prevented. Target normothermia with a core body temperature between 36 and 37.5 degrees Celsius in all post-arrest patients. For comatose children who do not follow commands after ROSC, the 2025 AHA guidelines recommend targeted temperature management at either normothermia or mild hypothermia of 32 to 34 degrees Celsius for 48 hours, followed by controlled rewarming at no faster than 0.5 degrees Celsius per hour. You should monitor core temperature continuously and not allow the patient to become febrile at any point during or after temperature management.
Both hypoglycemia and hyperglycemia worsen neurological outcomes after cardiac arrest and must be actively managed. You should check blood glucose immediately after ROSC and at frequent intervals to ensure you correct hypoglycemia without delay. Target a blood glucose level between 80 and 180 mg/dL. Avoid aggressive insulin therapy targeting tight glucose control, as hypoglycemia in the post-arrest period is more harmful than mild hyperglycemia. You must also correct electrolyte abnormalities, including sodium, potassium, calcium, and magnesium, as these directly affect cardiac and neurological function. Monitor serum lactate levels to assess tissue perfusion and guide ongoing resuscitation efforts.
Seizures are common after pediatric cardiac arrest and worsen neurological outcomes by increasing cerebral metabolic demand. Since both clinical and subclinical seizures occur in the post-arrest period, you should obtain continuous EEG monitoring in all comatose patients as soon as it becomes available. Treat clinical seizures immediately with benzodiazepines as the first-line agent and escalate to levetiracetam, fosphenytoin, or phenobarbital if seizures persist. Reassess neurological status at frequent intervals to document any changes in pupillary response or level of consciousness. Do not perform neurological prognostication within the first 72 hours after arrest, as the full extent of recovery cannot be accurately determined during this window.
Treating the physiological consequences of cardiac arrest is not enough. The underlying cause must be identified and addressed to prevent rearrest. Use the Hs and Ts framework to systematically investigate reversible causes, including hypoxia, hypovolemia, hypothermia, acidosis, electrolyte abnormalities, tension pneumothorax, cardiac tamponade, toxins, and thrombosis. Obtain a 12-lead ECG to identify any underlying arrhythmia, conduction abnormality, or ischemic change. Order targeted investigations based on the suspected cause, including chest imaging, point-of-care ultrasound, and laboratory studies. Based on the most likely etiology, you should consult the appropriate specialist early, whether in cardiology, toxicology, or infectious disease, to guide definitive management.
Once the patient is stabilized, you should arrange immediate transfer to a PICU for ongoing monitoring and management. Secure all active infusions, airway devices, and monitoring lines before transport. You must brief the receiving team on the arrest duration, initial rhythm, interventions performed, total fluid volume, medications given, and current hemodynamic and neurological status. After transfer, continue monitoring heart rate, blood pressure, SpO2, end-tidal CO2, temperature, glucose, and urine output at frequent intervals. Post-arrest patients can deteriorate rapidly, so maintain a low threshold for escalating care.
Pediatric and adult post-resuscitation care share the same physiological goals but differ significantly in target values, temperature management protocols, and neurological monitoring priorities. The table below outlines the key differences.
The PALS Post-Resuscitation Care Algorithm requires you to manage multiple physiological systems simultaneously in a time-sensitive environment. Oxygenation, hemodynamics, temperature, glucose, and neurological monitoring all require active intervention in the hours following ROSC. These are not skills that can be developed through reading alone. Post-resuscitation care scenarios are among the most cognitively demanding in PALS training because every decision affects neurological outcome.
Building that competency requires hands-on simulation in a structured clinical environment, not just familiarity with the steps. If you are preparing for initial PALS certification or an upcoming recertification, CPR Lifeline offers AHA-authorized PALS courses with pediatric-specific simulations covering the full resuscitation continuum, including post-resuscitation care.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
Titrate oxygen to maintain SpO2 between 94 and 99 percent after ROSC. Do not administer 100 percent oxygen routinely. Hyperoxia causes oxidative stress and worsens reperfusion injury to the brain and myocardium. Reduce FiO2 as soon as the patient is stable while maintaining the target SpO2 range.
Target a PaCO2 of 35 to 45 mmHg after ROSC. Hypocapnia from excessive ventilation causes cerebral vasoconstriction, reduces cerebral blood flow, and worsens neurological outcomes. Use continuous waveform capnography to monitor end-tidal CO2 and guide ventilation adjustments in real time to stay within this target range.
Target a blood glucose level between 80 and 180 mg/dL. Correct hypoglycemia immediately after ROSC. Avoid aggressive insulin therapy targeting tight glucose control, as hypoglycemia in the post-arrest period is more harmful than mild hyperglycemia. Check blood glucose at frequent intervals throughout the post-resuscitation period.
Targeted temperature management should be initiated as soon as possible after ROSC in comatose children who do not follow commands. The 2025 AHA guidelines recommend TTM at either normothermia of 36 to 37.5 degrees Celsius or mild hypothermia of 32 to 34 degrees Celsius. Prevent fever in all post-arrest patients regardless of whether formal TTM is initiated.
Targeted temperature management should be maintained for 48 hours in pediatric post-arrest patients. After 48 hours, controlled rewarming should begin at a rate no faster than 0.5 degrees Celsius per hour. Do not allow the patient to become febrile during or after rewarming, as hyperthermia worsens neurological outcomes.
Clinical seizures present with rhythmic limb movements, eye deviation, or facial twitching. Subclinical seizures produce no visible clinical signs and are only detectable on continuous EEG monitoring. Both types worsen neurological outcomes by increasing cerebral metabolic demand. Obtain continuous EEG monitoring in all comatose post-arrest patients and treat seizures immediately with benzodiazepines as the first-line agent.
Neurological prognostication should not be performed within the first 72 hours after cardiac arrest. The full extent of neurological recovery cannot be accurately determined during this window, particularly in patients undergoing targeted temperature management.

Home | About Us | Classes | Locations | Blogs | FAQ’s | Group Training | Contact Us
Copyright © 2025 cprlifeline. All Rights Reserved. Powered by Splendour Group
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!