
Septic shock is one of the most time-critical emergencies in pediatric care. Every minute without targeted intervention increases the risk of organ failure and death. The PALS Septic Shock Algorithm gives you a structured, evidence-based sequence to recognize septic shock early, stabilize the patient, and escalate treatment when the initial response is not enough.
Pediatric septic shock presents differently than it does in adults. Children compensate longer before showing obvious signs of deterioration, which makes early recognition harder and more important. This algorithm guides you through the first minutes of assessment, fluid resuscitation, antibiotic administration, and vasopressor therapy, so your response is systematic and without delay.

The PALS Septic Shock Algorithm is the AHA-developed protocol for identifying and managing septic shock in pediatric patients from infancy through adolescence. It defines septic shock as a life-threatening organ dysfunction caused by a dysregulated host response to infection, resulting in cardiovascular failure and inadequate tissue perfusion despite fluid resuscitation.
This PALS algorithm is structured around time-sensitive decision points. Your response in the first 15 minutes determines whether the patient stabilizes or deteriorates further. Each step builds on the previous assessment, moving from recognition and stabilization through fluid resuscitation, antibiotic administration, and vasopressor therapy. The goal at every stage is the same, which is to restore adequate perfusion to the organs before irreversible damage occurs.
The PALS Septic Shock Algorithm is time-driven. Each step carries a specific window for action, and delays at any point directly worsen patient outcomes. In a team-based setting, several interventions occur simultaneously. Below is the full step-by-step breakdown, starting from the moment you suspect septic shock in a pediatric patient.
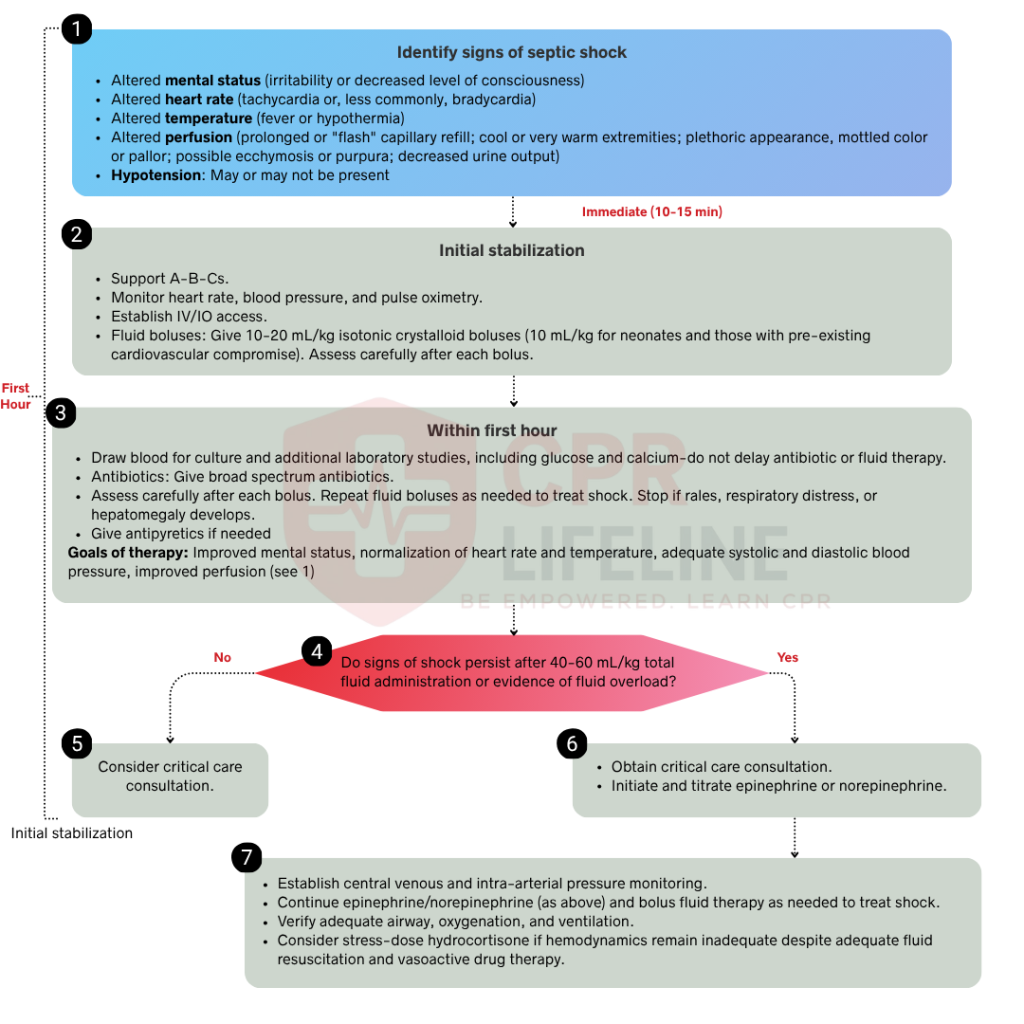
Early recognition is the most critical step in the algorithm. Children compensate for circulatory failure longer than adults, so obvious signs of shock can appear late. You must actively look for early indications such as tachycardia out of proportion to fever, altered mental status, prolonged or flash capillary refill, weak or bounding pulses, mottled or flushed skin, decreased urine output, and a suspected infection source. Do not wait for hypotension to confirm septic shock in a child. Hypotension is a late sign and indicates decompensated shock. Treat any child with tachycardia, altered perfusion, and a suspected infection source as septic shock until proven otherwise. Once you identify these signs, move immediately to Step 2.
Once septic shock is identified, act immediately. Open and maintain the airway, provide high-flow oxygen to maintain SpO2 above 94%, and attach continuous cardiac monitoring, pulse oximetry, and a blood pressure cuff. Establish IV or IO access without delay, transitioning immediately to an IO needle if peripheral attempts are unsuccessful after two tries or 90 seconds. During this process, draw initial labs and correct any existing hypoglycemia before moving directly to the next phase of the resuscitation algorithm.
The first hour of septic shock management is the highest-impact window for patient survival. The AHA refers to this as the golden hour, where early, aggressive intervention significantly improves outcomes. Three actions must occur rapidly and, in a team-based setting, simultaneously.
Begin fluid resuscitation immediately after establishing access by administering an isotonic crystalloid, such as normal saline or lactated Ringer’s, at a dose of 20 mL/kg over 5 to 10 minutes. Reassess perfusion after each bolus, repeating the process up to a total of 60 mL/kg within the first hour if signs of shock persist. Stop fluid administration immediately if the patient shows signs of fluid overload, such as new crackles during lung auscultation, increased work of breathing, or hepatomegaly.
Draw blood cultures before administering antibiotics, but never delay treatment to obtain them. Administer broad-spectrum antibiotics within 60 minutes of septic shock recognition, with selection based on the suspected infection source, patient age, and local resistance patterns. As early antibiotic administration is one of the strongest independent predictors of survival, rapid delivery is a critical priority in the stabilization process.
Reassess the patient after each fluid bolus and at the end of the first hour to evaluate the clinical response. Look for improvements in heart rate, capillary refill, mental status, urine output, and blood pressure. If perfusion normalizes, you may proceed to Step 4. If signs of shock persist despite adequate fluid resuscitation, move immediately to Step 5.
Normalizing perfusion after fluid resuscitation indicates that the immediate threat is controlled, but not eliminated. Because septic shock can recur rapidly if the underlying infection is undertreated or fluid balance shifts, you must consult a pediatric critical care specialist and arrange a PICU transfer immediately. Continue frequent monitoring of heart rate, blood pressure, capillary refill, mental status, and urine output while ensuring antibiotics remain on schedule and vascular access is maintained until the final handoff to the critical care team.
If shock persists after 60 mL/kg of fluid resuscitation, transition immediately to vasopressor therapy, as fluid alone is no longer sufficient. For cold shock, initiate an epinephrine infusion at 0.1 mcg/kg per minute, titrating up to 1 mcg/kg per minute based on the perfusion response. In cases of warm shock, norepinephrine is the preferred first-line agent, starting at 0.1 mcg/kg per minute and titrated to effect. Dopamine remains an alternative at 2 to 20 mcg/kg per minute if other vasopressors are unavailable. All vasopressors must be administered as continuous infusions and never as boluses. Continuously reassess perfusion after initiation and consult pediatric critical care immediately to coordinate advanced management.
Once vasopressor therapy is initiated, your focus shifts to maintaining stability and preventing secondary deterioration. Reassess perfusion markers every 15 to 30 minutes, including heart rate, blood pressure, capillary refill, mental status, and urine output. Target a urine output of at least 1 mL/kg per hour. Recheck lactate levels to confirm tissue perfusion is improving. If lactate remains elevated despite vasopressor therapy, escalate to pediatric critical care immediately. Continue broad-spectrum antibiotics and narrow coverage once culture results are available. Secure a central venous line for ongoing vasopressor administration and hemodynamic monitoring if not already placed.
Pediatric septic shock presents in two distinct hemodynamic patterns. Identifying which type you are dealing with directly determines your vasopressor choice in Step 5. Both types share the same underlying cause, which is infection-driven cardiovascular failure, but they differ significantly in clinical presentation.
Warm shock occurs when the cardiovascular system responds to infection with increased cardiac output and peripheral vasodilation. The body is attempting to compensate by pumping more blood, but the vessels are too dilated to maintain adequate perfusion pressure.
You recognize warm shock by these 4 clinical features:
Norepinephrine is the first-line vasopressor for warm shock. It restores vascular tone without excessively increasing heart rate.
Cold shock occurs when the cardiovascular system fails to compensate, resulting in decreased cardiac output and peripheral vasoconstriction. The body is redirecting blood away from the periphery to protect the vital organs.
You recognize cold shock by these 4 clinical features:
Epinephrine is the first-line vasopressor for cold shock. It increases both heart rate and myocardial contractility to restore cardiac output.
Medications used in the PALS Septic Shock Algorithm have a specific indication, dose, and route. Your choice of medication depends on the type of shock, the patient’s response to fluids, and whether first-line agents have failed.
The PALS Septic Shock Algorithm requires you to recognize subtle early signs, make rapid fluid and vasopressor decisions, and escalate care without hesitation. These are high-stakes, time-critical skills that reading alone cannot build. Pediatric septic shock is one of the most complex scenarios covered in PALS training, and simulation-based practice is the only way to develop the clinical confidence this algorithm demands.
PALS certification through the American Heart Association is required for physicians, nurses, paramedics, and respiratory therapists managing pediatric emergencies. Certification is valid for two years. If you are preparing for initial certification or an upcoming recertification, CPR Lifeline offers AHA-authorized PALS courses with pediatric-specific simulations covering every algorithm, including septic shock, bradycardia, and cardiac arrest.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
Early signs include tachycardia out of proportion to fever, altered mental status, prolonged or flash capillary refill, weak or bounding peripheral pulses, mottled or flushed skin, and decreased urine output. Do not wait for hypotension to act. In children, hypotension is a late sign of decompensated shock.
Warm shock presents with bounding pulses, flash capillary refill, and warm flushed skin, caused by peripheral vasodilation and high cardiac output. Cold shock presents with weak pulses, prolonged capillary refill, and cool mottled skin, caused by low cardiac output and peripheral vasoconstriction. The distinction determines your vasopressor choice. Norepinephrine is used for warm shock and epinephrine for cold shock.
Administer isotonic crystalloid at 20 mL/kg IV or IO over 5 to 10 minutes per bolus. Repeat boluses up to a total of 60 mL/kg in the first hour if shock persists. Reassess perfusion after each bolus and stop fluid administration if signs of fluid overload develop, including new crackles, increased work of breathing, or hepatomegaly.
Start vasopressors when shock persists after 60 mL/kg of fluid resuscitation. Epinephrine is the first-line agent for cold shock and norepinephrine for warm shock. Both are administered as continuous IV or IO infusions. Never give vasopressors as a bolus dose.
Antibiotic selection depends on the suspected infection source, patient age, and local resistance patterns. Broad-spectrum coverage is initiated within 60 minutes of recognizing septic shock. Blood cultures must be drawn before administration, but antibiotic delivery should never be delayed to obtain them. Narrow antibiotic coverage once culture and sensitivity results are available.
Hydrocortisone is a third-line intervention reserved for catecholamine-resistant septic shock, where the patient does not respond to maximum doses of epinephrine or norepinephrine. It is not a routine first or second-line medication. The loading dose is 1 to 2 mg/kg IV or IO, up to a maximum of 100 mg, followed by continuous or intermittent dosing based on clinical response.

Home | About Us | Classes | Locations | Blogs | FAQ’s | Group Training | Contact Us
Copyright © 2025 cprlifeline. All Rights Reserved. Powered by Splendour Group
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!