Pediatric emergencies require more precision than standard care because children have unique needs. Children are not just small adults, their physiology, emergency presentations, and treatment responses differ in ways that require a dedicated, evidence-based framework. The Pediatric Advanced Life Support (PALS) Algorithm is a structured, decision-based protocol developed by the American Heart Association to guide trained providers through the recognition and management of life-threatening emergencies in infants and children. From respiratory failure to cardiac arrest and shock, the PALS Algorithm gives you a clear, stepwise pathway to follow when the stakes are highest.
This page covers the complete PALS Algorithm based on the 2025 AHA guidelines, including all core algorithms, key protocol updates, systematic assessment, and clinical considerations specific to pediatric patients.
The PALS Algorithm is a set of evidence-based clinical protocols developed by the American Heart Association to standardize the emergency care of critically ill infants and children. It provides structured decision pathways for assessing and managing conditions including respiratory distress, respiratory failure, shock, and cardiac arrest in pediatric patients.
Unlike BLS, PALS extends into clinical management by integrating systematic assessment, targeted interventions, and medication administration. This algorithm is essential because pediatric cardiac arrest typically results from respiratory failure or shock rather than primary cardiac events. Identifying these signs early can stop a child’s condition from getting worse. Designed for high-stress environments, PALS uses weight-based treatments adjusted to a child’s specific needs. Providers trained in this structured framework demonstrate faster recognition and more accurate interventions, leading to significantly better patient outcomes.

PALS is applied any time an infant or child presents with a condition that threatens normal breathing, circulation, or neurological function. The protocol is designed for the critical window where early, structured intervention has the greatest impact on survival and neurological recovery.
The primary situations that require PALS are:
When a child has no pulse or breathing, immediately start high-quality CPR. Use the Pediatric Cardiac Arrest Algorithm to manage rhythms with precise medications and interventions.
If a child has an abnormal heart rate with poor perfusion, you must determine if the rhythm is causing the instability and then follow the correct PALS intervention pathway based on how the rhythm is classified.
If a child shows signs of increased breathing effort, abnormal airway sounds, or poor ventilation, you must quickly identify the cause. Acting fast can stop these issues from progressing into respiratory arrest, which is the most common precursor to pediatric cardiac arrest.
If a child's circulatory system fails to deliver enough oxygen to their tissues, you must act quickly. PALS helps you recognize distributive, hypovolemic, obstructive, or cardiogenic shock and provides specific fluid and medication pathways for each type.
When a child shows signs of circulatory failure driven by infection, you must act fast to reverse the shock. PALS provides a specific algorithm covering early fluid resuscitation, the right vasopressors, and timely antibiotics to stop organ damage before it becomes permanent.
Once a child achieves ROSC after cardiac arrest, you must shift from active resuscitation to systematic stabilization. PALS guides you through managing oxygen levels, blood flow, glucose, and temperature to protect neurological status and ensure a steady recovery.
PALS certification is required for healthcare providers who work in environments where they may encounter critically ill or injured infants and children. The following roles are commonly required to hold a current AHA PALS certification:
The 2025 AHA guidelines organize PALS into five core algorithms. Each one addresses a specific life-threatening condition in pediatric patients. Knowing which algorithm applies to your patient’s presentation is the first step toward delivering a structured and effective response.
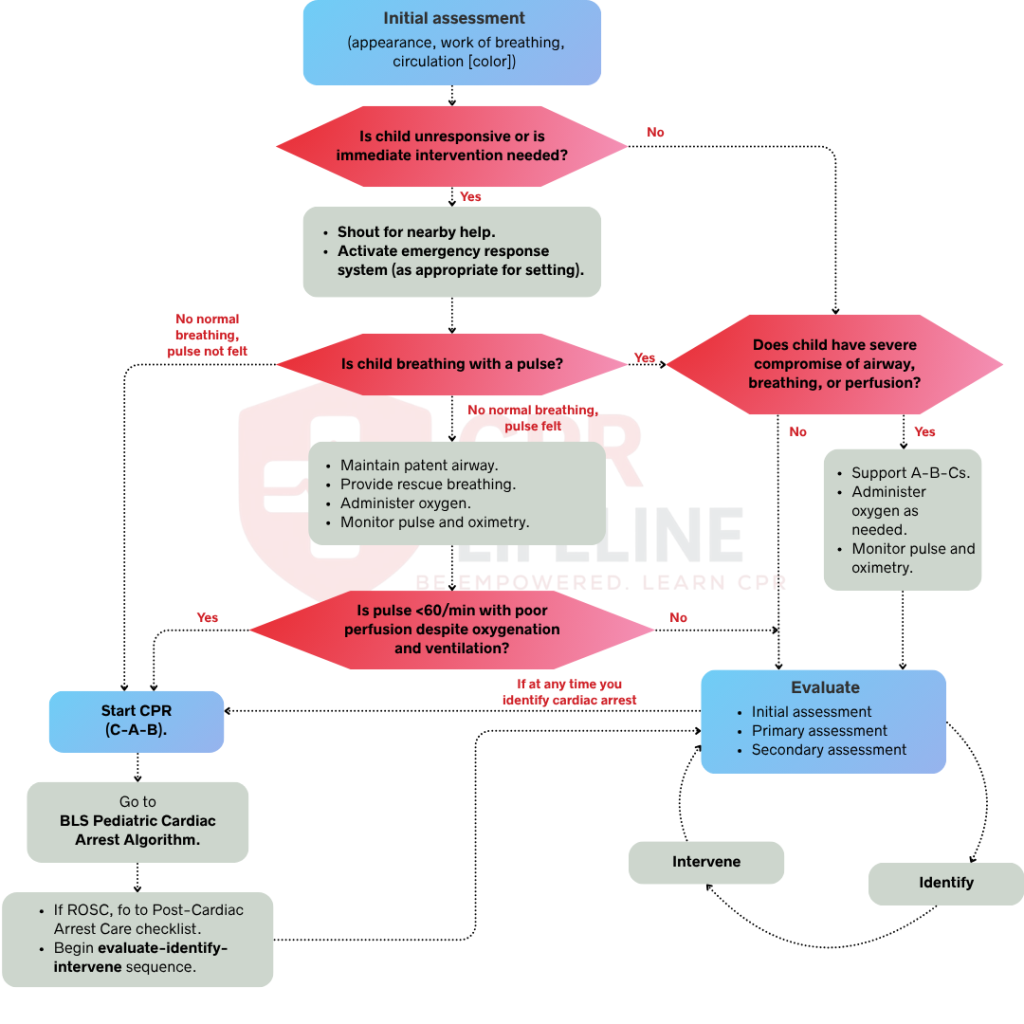
The PALS Systematic Approach Algorithm provides the foundational assessment framework applied before any other PALS algorithm is initiated. It directs providers through a structured sequence covering initial impression, primary assessment using the ABCDE approach, and secondary assessment. This algorithm ensures that life-threatening conditions are identified in the correct order of priority before targeted interventions begin.
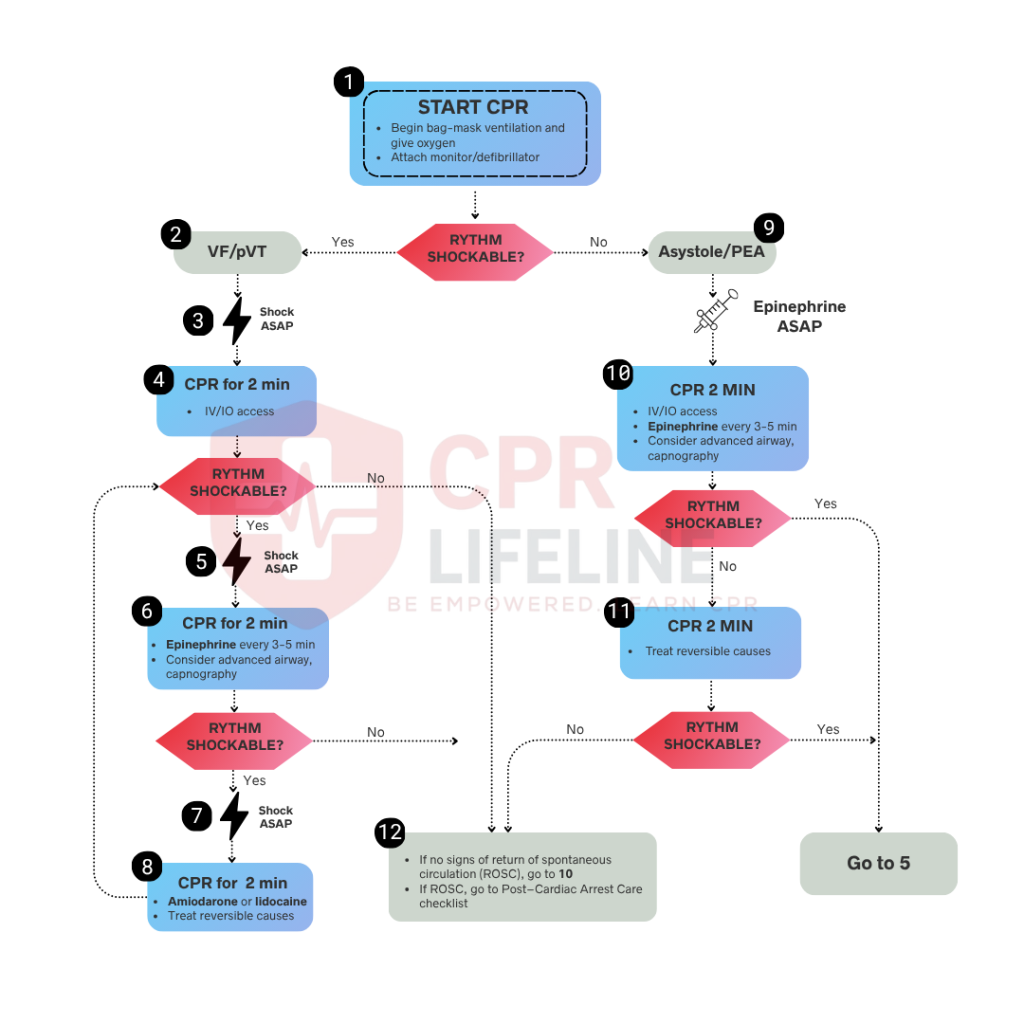
The Pediatric Cardiac Arrest Algorithm guides providers through cardiac arrest management in infants and children. It covers rhythm identification, high-quality CPR, defibrillation for shockable rhythms, and medication administration for both shockable and non-shockable pathways. In cases of ventricular fibrillation or pulseless ventricular tachycardia, immediate defibrillation combined with uninterrupted CPR is the priority intervention.
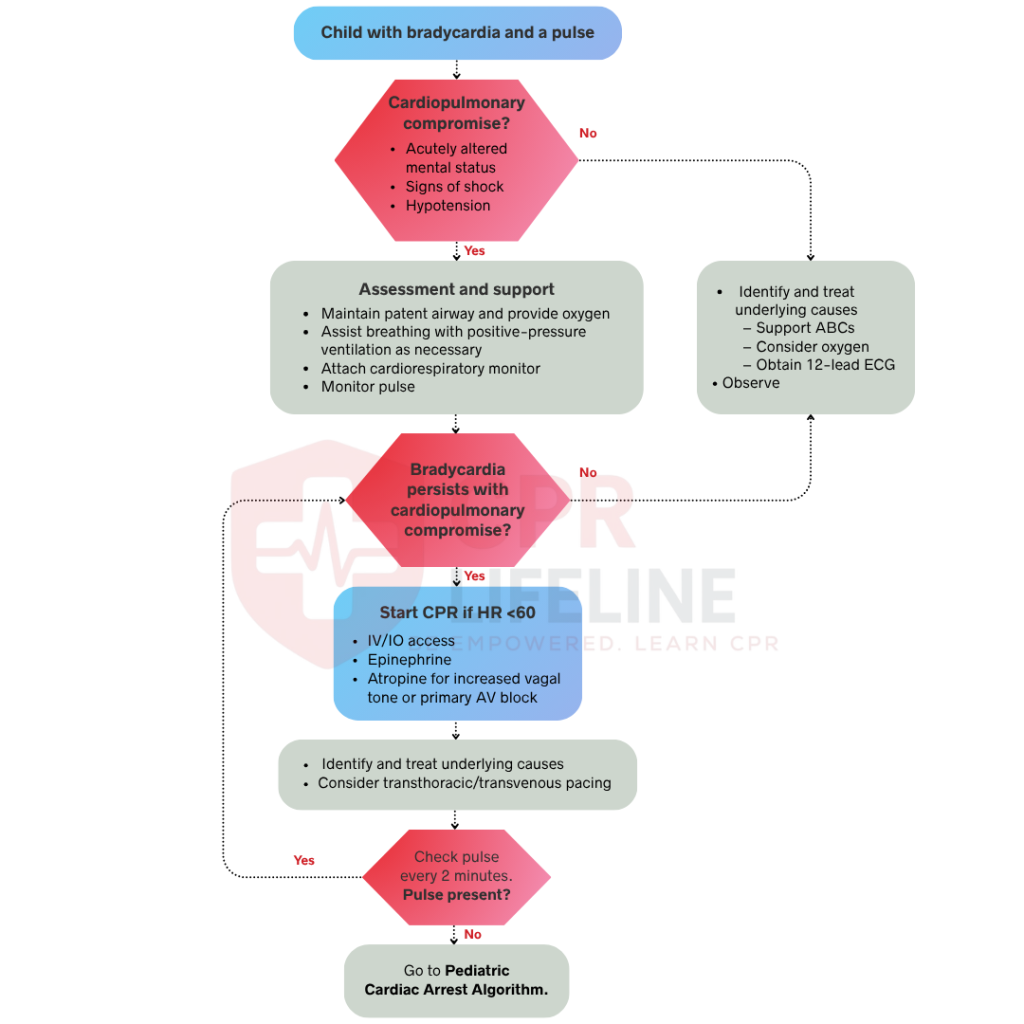
The Pediatric Bradycardia Algorithm guides providers through the assessment and management of symptomatic bradycardia in pediatric patients with a pulse. It applies when the heart rate falls below normal for age with signs of hemodynamic compromise. When bradycardia persists despite adequate oxygenation, the algorithm directs providers toward epinephrine administration and emergency pacing.
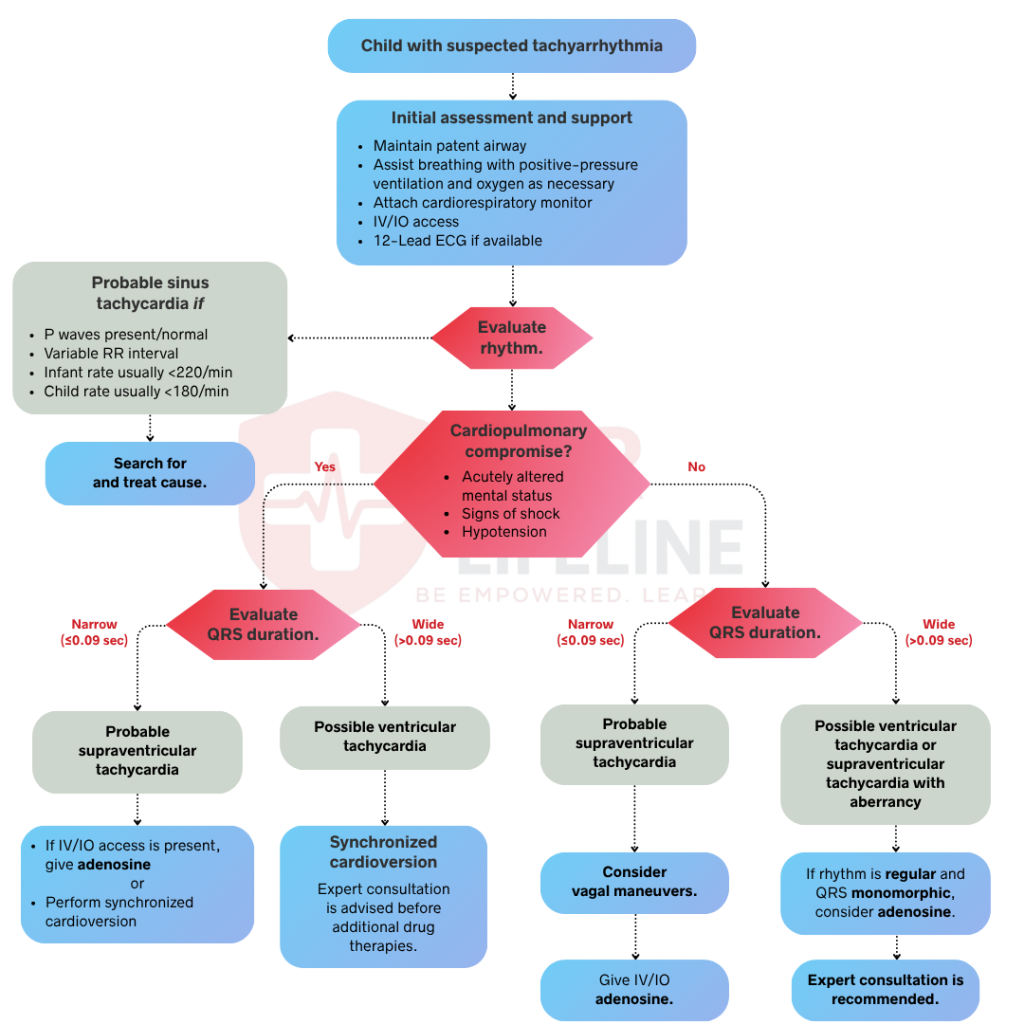
The Pediatric Tachycardia Algorithm guides providers through the evaluation and treatment of abnormally fast heart rates in pediatric patients with a pulse. It directs providers to distinguish between sinus tachycardia and pathological rhythms. Unstable patients require immediate synchronized cardioversion, while stable patients are managed through vagal maneuvers or pharmacological intervention based on rhythm classification.
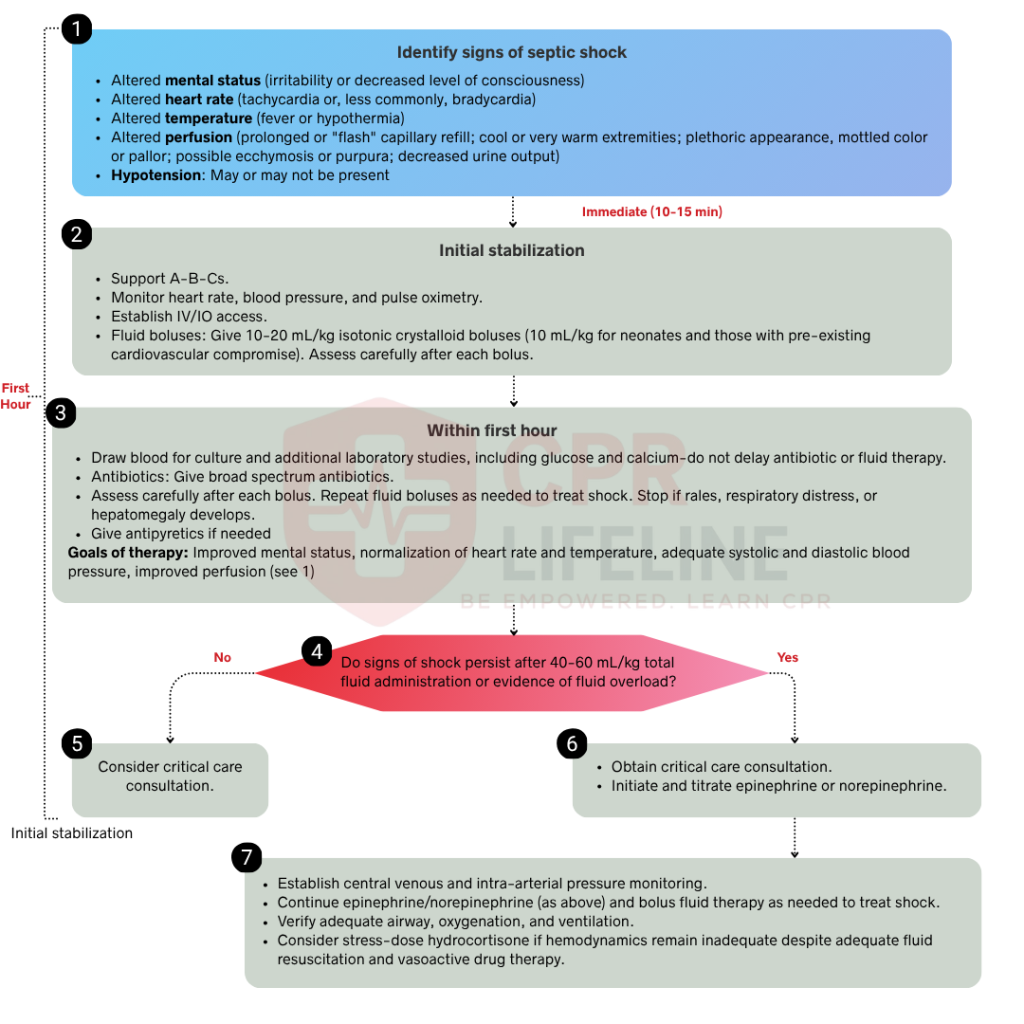
The Pediatric Septic Shock Algorithm guides providers through the recognition and treatment of septic shock in infants and children. It covers fluid resuscitation, vasopressor selection, and antibiotic timing. When the patient fails to respond to initial fluid boluses, the algorithm directs providers toward vasoactive medication initiation to restore perfusion pressure before organ dysfunction develops.
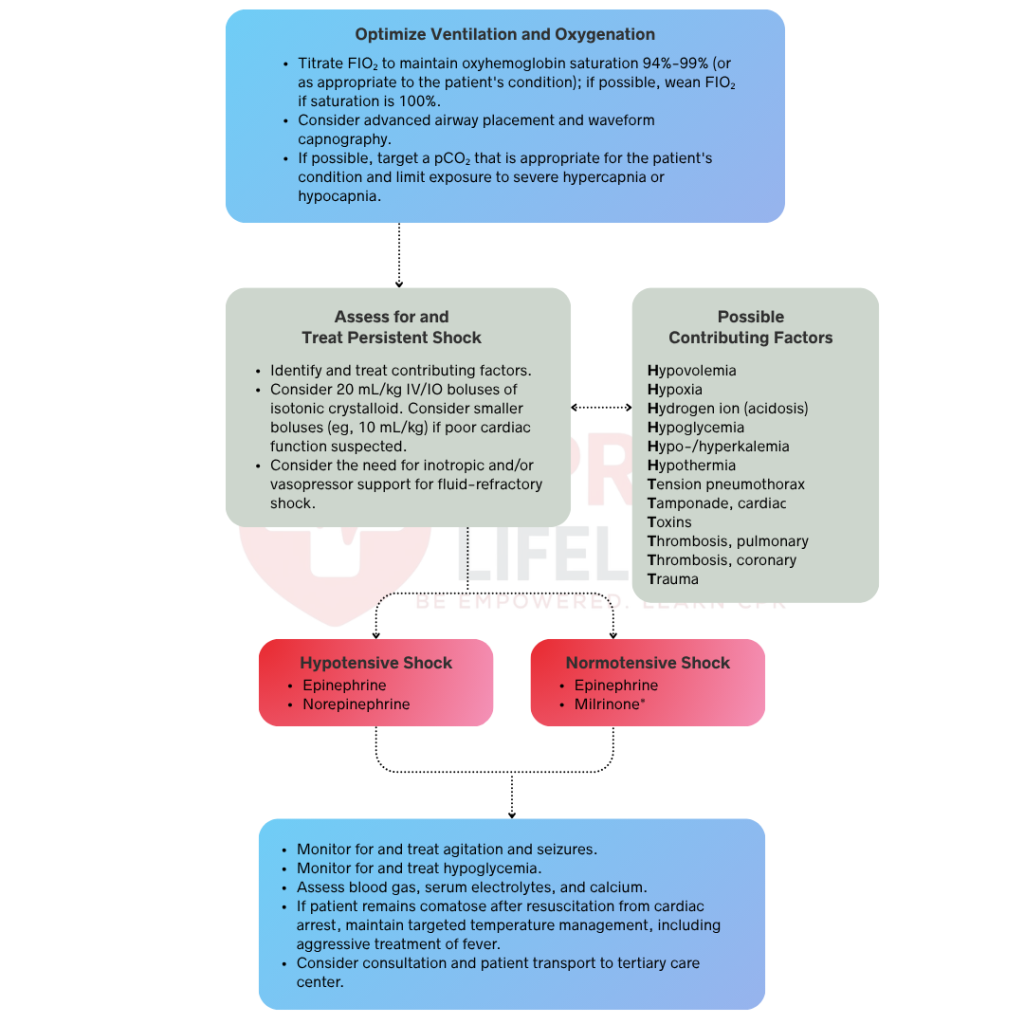
The Pediatric Post-Resuscitation Care Algorithm outlines the stabilization of pediatric patients following return of spontaneous circulation. It directs providers through oxygenation, hemodynamic support, glucose management, temperature control, and neurological monitoring. When a cardiac or metabolic cause is suspected, the algorithm guides targeted diagnostic workup to maximize neurological recovery.
The AHA released updated PALS guidelines back in October 2025. These updates reflect the latest pediatric resuscitation research and refine how providers assess and manage critically ill infants and children. Here are the most important changes:
Compressions must be delivered at 100 to 120 per minute at a depth of at least one-third of the chest diameter. Providers must maintain a compression fraction above 60% and use real-time feedback devices to monitor and correct technique during resuscitation.
Recent updates enhance the management of advanced airway usage, ventilation rates, and strategies to prevent hyperventilation. Bradycardia and tachycardia algorithms refine pharmacologic escalation, pacing initiation, and cardioversion timing for stable versus unstable rhythms.
Targeted temperature management parameters are clarified for pediatric patients, with strict guidance on avoiding both hyperthermia and aggressive hypothermia. Hemodynamic targets, oxygenation limits, and glucose thresholds are more precisely defined to reduce secondary brain injury during recovery.
The 2025 guidelines introduce measurable perfusion targets during CPR. When invasive monitoring is available, providers should target a diastolic blood pressure of at least 25 mmHg in infants and at least 30 mmHg in older children during active compressions.
The systematic approach to PALS provides a structured framework for assessing and managing critically ill pediatric patients. It prioritizes rapid identification of life-threatening conditions through a consistent, repeatable sequence that prevents critical steps from being missed under pressure.
Applying the PALS Algorithm effectively requires more than memorizing the steps. Several clinical principles directly impact the quality of care you deliver during a pediatric emergency. These considerations apply across all PALS scenarios regardless of the specific algorithm in use.
The sooner you identify signs of respiratory distress, shock, or cardiac arrest in a pediatric patient, the greater the chance of preventing deterioration into a more critical state. Watch for subtle early indicators including changes in breathing pattern, skin color, level of consciousness, and muscle tone. Acting at the compensated stage of shock or early respiratory distress gives you the greatest clinical advantage before the child decompensates.
Effective team communication reduces errors during pediatric resuscitation. Use closed-loop communication by assigning tasks clearly, confirming instructions verbally, and reporting back upon completion. Designating roles before resuscitation begins prevents task duplication and ensures no step is missed, keeping the team focused under high-stress conditions.
Calibrate every PALS intervention to the child’s age and weight. Medication doses, defibrillation energy levels, and equipment sizes vary significantly from neonates to adolescents. Use a length-based tool like the Broselow tape if the weight of the patient is unknown. Applying adult sizes or doses to pediatric patients can cause direct harm and reduce the effectiveness of your care.
Confirm that correctly sized pediatric equipment is available and ready before resuscitation begins. This includes appropriately sized bag-mask devices, airway adjuncts, defibrillator pads, and endotracheal tubes. Using the wrong equipment size compromises airway management and reduces CPR effectiveness, and introduces unnecessary risk during a time-critical emergency.
Knowing normal pediatric vital signs is essential for recognizing early deterioration in critically ill infants and children. The values below are based on the 2025 AHA PALS guidelines and serve as the clinical reference points used across all PALS assessment and intervention decisions.
Oxygen Saturation (SpO2): Normal SpO2 is above 94% for pediatric patients breathing room air. Values below 90% indicate hypoxemia and require immediate intervention. Visible cyanosis of the skin, lips, or nail beds typically appears once saturation drops below this level, signaling a critical need for oxygenation.
Temperature: Normal body temperature in pediatric patients ranges from 36°C to 38°C. Hypothermia, defined as a temperature below 36°C, increases resuscitation difficulty and mortality risk. Hyperthermia above 38.5°C may indicate infection, neurological injury, or heat-related illness, requiring prompt evaluation and management within the PALS framework.
Identifying and treating reversible causes is one of the most critical actions during pediatric cardiac arrest. The H’s and T’s provide a systematic framework for evaluating these causes during active resuscitation. Addressing a reversible cause directly changes the clinical outcome and must be pursued simultaneously alongside high-quality CPR.


PALS certification requires active BLS certification and a working knowledge of pediatric assessment, rhythm recognition, and pharmacology. The course validates your ability to apply PALS algorithms in real pediatric emergencies across in-hospital and out-of-hospital settings.
The PALS Algorithm converts decades of pediatric resuscitation research into clear, actionable steps that directly improve outcomes in the most critical moments of a child's care. The 2025 AHA guidelines sharpen every stage of the protocol, from systematic assessment to targeted intervention and post-arrest recovery. Learning these algorithms equips you to act decisively, accurately, and without hesitation when every second matters. For providers looking to build and validate these skills, AHA PALS certification is available at CPR Lifeline locations across Tennessee and Georgia. Find a location near you and complete your PALS certification on your schedule.
Support Available
Passed rate
Certified Students
The PALS Algorithm is a set of evidence-based clinical protocols developed by the American Heart Association to guide trained providers through life-threatening emergencies in infants and children. It provides structured decision pathways for managing cardiac arrest, respiratory failure, shock, and arrhythmias in pediatric patients across in-hospital and out-of-hospital settings.
BLS covers the immediate life-saving actions of CPR, AED use, and airway management for patients of all ages. PALS extends these skills into broader clinical management for critically ill pediatric patients, including systematic assessment, rhythm-specific interventions, weight-based medications, and specialized post-resuscitation care.
The core PALS algorithms are the PALS Systematic Approach Algorithm, Pediatric Cardiac Arrest Algorithm, Pediatric Bradycardia with a Pulse Algorithm, Pediatric Tachycardia with a Pulse Algorithm, Pediatric Septic Shock Algorithm, and Pediatric Post-Resuscitation Care Algorithm. Each addresses a specific life-threatening condition in pediatric patients.
Epinephrine is administered every 3 to 5 minutes during pediatric cardiac arrest at a dose of 0.01 mg/kg IV or IO. The maximum single dose is 1 mg. Epinephrine is indicated for all cardiac arrest rhythms including ventricular fibrillation, pulseless ventricular tachycardia, asystole, and pulseless electrical activity.
The reversible causes are organized into the H’s and T’s framework. The 5 H’s are Hypoxia, Hypovolemia, Hydrogen ions, Hypo and Hyperkalemia, and Hypothermia. The 5 T’s are Toxins, Tamponade, Tension Pneumothorax, Thrombosis Pulmonary, and Thrombosis Coronary. Identifying and treating a reversible cause during active resuscitation directly improves the chance of survival.

Home | About Us | Classes | Locations | Blogs | FAQ’s | Group Training | Contact Us
Copyright © 2025 cprlifeline. All Rights Reserved. Powered by Splendour Group
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!
