Cardiac arrest in pregnancy is one of the most challenging emergencies in medicine. You are simultaneously responsible for two lives, and standard ACLS protocols alone are not enough. The physiological changes of pregnancy, including aortocaval compression, increased oxygen demand, and a difficult airway, require specific modifications to your resuscitation approach.
The 2025 AHA Cardiac Arrest in Pregnancy Algorithm outlines a precise, time-sensitive approach to maternal resuscitation. Understanding each step, from team activation to resuscitative delivery, gives you the clinical foundation to act decisively when both lives depend on it.

The Cardiac Arrest in Pregnancy Algorithm provides a structured framework for in-hospital maternal resuscitation. This algorithm integrates standard ACLS principles with pregnancy-specific modifications. You will follow a systematic approach that addresses the unique challenges of maternal cardiac arrest. The algorithm emphasizes simultaneous interventions rather than sequential steps.
The algorithm contains critical pregnancy-specific components including uterine displacement, airway management, cause identification using the A-H framework, and resuscitative delivery with a strict five-minute target. The primary goal of this algorithm is effective maternal resuscitation which is built on the principle that improving maternal outcomes is the most reliable way to improve fetal outcomes.
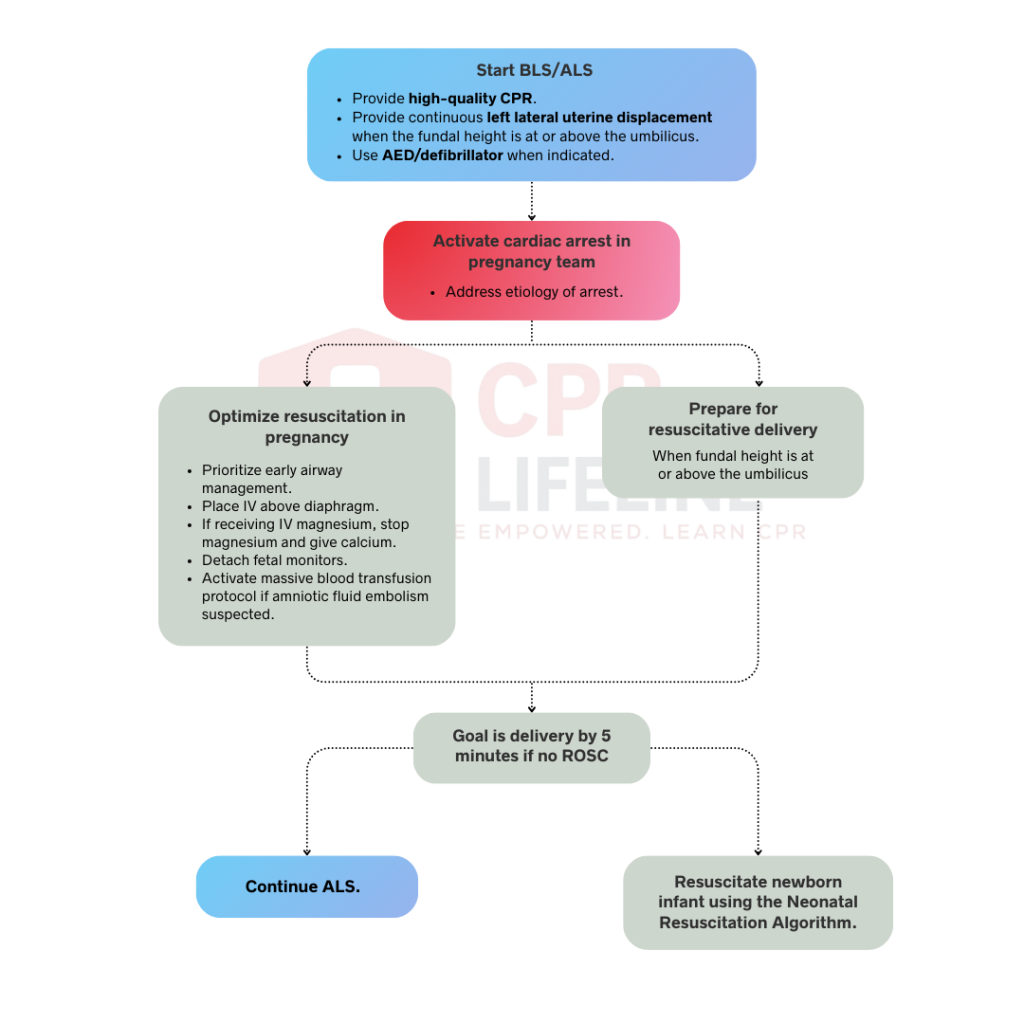
The algorithm follows a clear sequence. Each step builds on standard ACLS while adding pregnancy-specific modifications.
To handle a maternal cardiac arrest effectively, you should begin high-quality CPR immediately by pushing hard and fast at a rate of 100 to 120 compressions per minute. It is vital to allow for full chest recoil between every single compression while keeping any interruptions to less than 10 seconds, as this constant flow is necessary to maintain enough perfusion for both the mother and the baby.
If the fundal height has reached the umbilicus, a team member must provide continuous manual left lateral uterine displacement to relieve pressure on the major blood vessels during those compressions. You should still use your AED or defibrillator according to standard protocols since pregnancy does not change the energy levels or pad placement, though you must remember to remove any fetal monitors before delivering a shock.
Do not wait to see if standard resuscitation works and call for your specialized team immediately. Activating them early ensures that the right experts and the necessary equipment are at the bedside the moment things get critical. Once the team arrives, begin by identifying the underlying cause using the A-H framework. The goal for everyone is to start troubleshooting potential etiologies from the very second they walk through the door.
To give your patient the best chance at a successful resuscitation, you need to move quickly on several key interventions which are as follows:
Resuscitative delivery is indicated as soon as the fundal height reaches the umbilicus or higher. Your primary goal is to achieve delivery within five minutes of the initial cardiac arrest if ROSC has not yet occurred. Begin all necessary preparations by the four-minute mark to ensure the obstetrician can complete the procedure on time. This intervention is critical because it immediately relieves aortocaval compression and improves venous return to the maternal heart, which significantly increases the likelihood of a successful resuscitation.
Maternal survival remains the first priority while fetal viability is a secondary consideration during these efforts. Relieving the pressure on the major vessels is what allows your resuscitation techniques to actually work. You must perform the delivery at the exact location where the cardiac arrest occurred rather than attempting to move the patient to an operating room. Whether the patient is in the emergency department, the ICU, or a labor unit, the bedside is the only appropriate place to avoid wasting these critical minutes.
Standard ACLS medications and interventions should continue without interruption throughout the entire resuscitation process. You should administer epinephrine every three to five minutes while simultaneously treating any reversible causes and managing arrhythmias. It is vital to remember that your resuscitation efforts do not pause for the delivery itself. High-quality CPR must continue during and after the cesarean delivery to maintain maternal circulation and support the best possible outcome.
The neonatal team must be ready to receive the infant immediately and follow the standard Neonatal Resuscitation Program algorithm. Depending on the situation, the newborn may require anything from simple warming, drying, and stimulation to more intensive measures like positive pressure ventilation or chest compressions. While on-time delivery significantly improves outcomes for the newborn, it is essential that neonatal care does not distract the team from the ongoing maternal resuscitation. Both efforts should happen in parallel to ensure that the mother receives the continuous, high-quality support necessary for her own survival.
Two critical interventions distinguish maternal cardiac arrest resuscitation from standard ACLS protocols by directly addressing the unique physiology of pregnancy. Left uterine displacement relieves aortocaval compression during CPR, while resuscitative delivery removes this mechanical obstruction entirely to improve maternal circulation and provide the infant a chance at survival. You must master the correct technique for both maneuvers and understand the precise timing required to initiate them during the first few minutes of an arrest.
Effective uterine displacement requires one or two hands to manually shift the uterus toward the patient’s left side, typically with the provider standing on the patient’s left and pushing from the right. This manual technique is far superior to using a left lateral tilt wedge because wedges often destabilize the torso and decrease the quality of chest compressions.
By opting for manual displacement, the team maintains optimal compression depth and effectiveness while still successfully relieving aortocaval compression. To ensure this remains consistent, the team member assigned to this task must remain in position throughout the entire resuscitation and should not rotate into other roles.
Resuscitative delivery, also known as a perimortem cesarean, is a time-critical emergency procedure performed during maternal cardiac arrest. To maximize survival, you must initiate the incision by four minutes and complete the delivery by the five-minute mark. Performing this at the bedside immediately relieves pressure on major vessels, potentially increasing maternal cardiac output by up to 80% while giving the newborn the best chance at life.
The procedure prioritizes speed over cosmetics, typically utilizing a rapid vertical midline incision to deliver the infant and placenta. Throughout the surgery, the team must maintain high-quality CPR and airway management without any interruptions. The team leader should clearly announce time milestones, ensuring the obstetrician and neonatal team are synchronized while the bedside staff continues the standard ACLS algorithms for the mother.
Cardiac arrest in pregnancy has its distinct causes. You must identify and treat the underlying etiology while performing resuscitation. The A-H mnemonic helps you remember pregnancy specific and general causes.
ROSC is not the end of the resuscitation. Continue providing advanced life support and treat underlying causes.
Identify and fix the arrest's trigger immediately. Use transfusions for bleeding, calcium for magnesium toxicity, or aggressive support for embolism to prevent a recurrence.
Consider targeted temperature management while noting limited evidence in pregnancy. Consult your intensive care team early to set appropriate recovery goals for the mother.
If the patient is still pregnant, use continuous fetal heart rate monitoring to assess well-being. Regular obstetric consultation will guide your next management steps.
The neonatal team must manage the newborn’s resuscitation and determine the care level. This often includes NICU admission, therapeutic hypothermia, or other advanced interventions.
The cardiac arrest in pregnancy algorithm is your best opportunity to save two lives simultaneously. While understanding the foundational knowledge on paper is a great start, real-world success requires the ability to execute these steps with total confidence under extreme pressure. Every modification you implement, from uterine displacement to the five-minute delivery window, plays a massive role in the final outcome.
At CPR Lifeline, we offer official American Heart Association ACLS courses that prepare you to handle maternal cardiac arrest and other critical emergencies. Our flexible blended learning format allows you to complete the online curriculum at your own pace before attending a quick in-person skills session. Strengthen your emergency skills and gain the confidence to lead maternal resuscitation teams effectively.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
Pregnancy introduces physiological changes like aortocaval compression and higher oxygen demand. You must apply specific modifications to standard protocols to address these unique maternal requirements effectively.
Initiate delivery if the fundus reaches the umbilicus. You should begin the incision within four minutes and complete the delivery within five minutes of the arrest.
Compression of the inferior vena cava can block medications from reaching the heart. Use antecubital or jugular sites to ensure drugs circulate effectively during maternal resuscitation.
The A-H mnemonic identifies pregnancy-specific arrest causes like anesthesia, bleeding, cardiovascular events, and embolism. It ensures you systematically evaluate reversible triggers unique to the pregnant patient.
Yes, you must perform high-quality chest compressions without interruption throughout the cesarean procedure. Continuous circulation is vital for maternal stability and the best possible clinical outcome.
Address the underlying cause, monitor fetal heart rate, and manage maternal temperature. You should also facilitate the immediate transition of the newborn to a neonatal specialist team.

Home | About Us | Classes | Locations | Blogs | FAQ’s | Group Training | Contact Us
Copyright © 2025 cprlifeline. All Rights Reserved. Powered by Splendour Group
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!