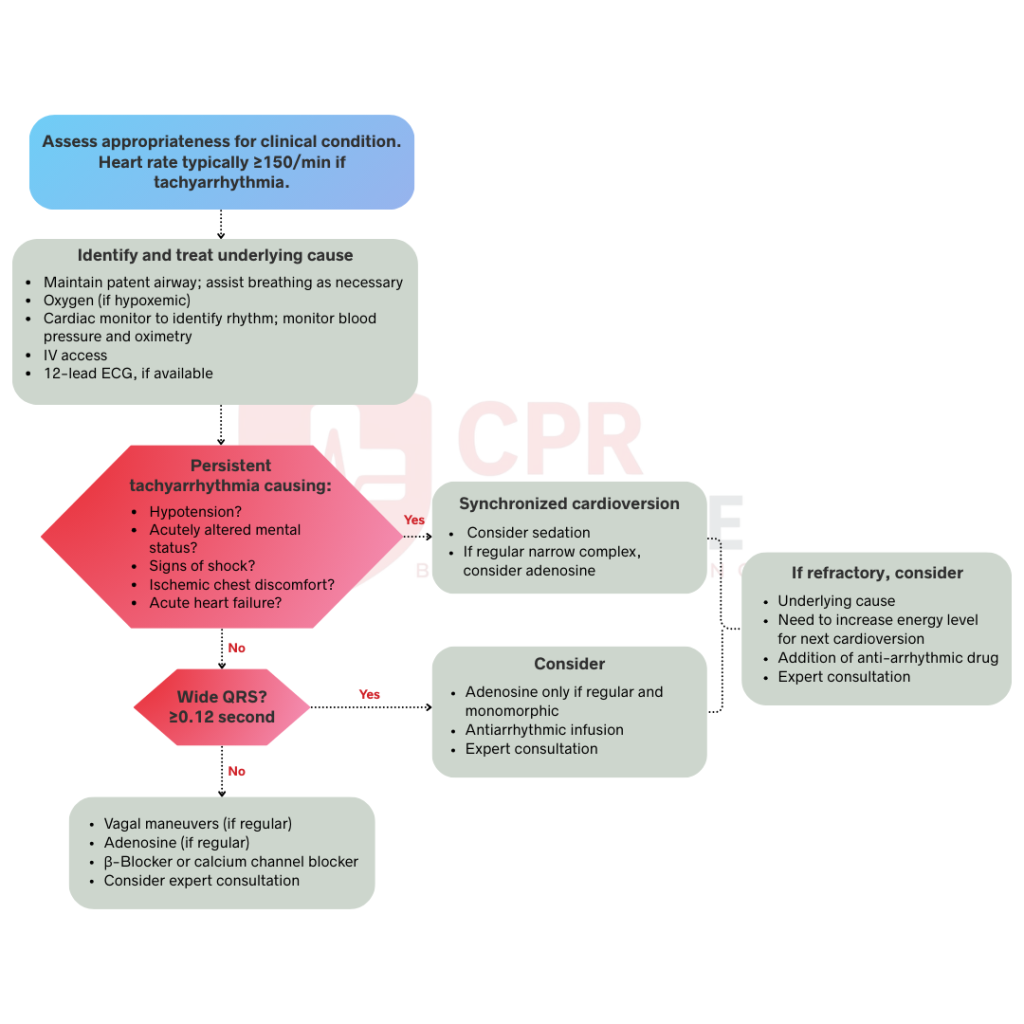
The ACLS tachycardia algorithm is a systematic, evidence-based protocol published and regularly updated by the American Heart Association that guides medical teams through the rapid assessment and treatment of patients with too fast heart rates. While tachycardia is technically defined as any heart rate above 100 beats per minute, the algorithm becomes clinically relevant at heart rates above 150 bpm, where hemodynamic compromise is far more likely to occur. The entire protocol revolves around one critical decision point, which is whether the patient is hemodynamically stable or unstable, and that distinction drives every treatment decision that follows.
Here we walk through the most current 2025 AHA Tachycardia Guidelines and walk you through rhythm identification, stable and unstable tachycardia management, medication dosing, and when to escalate care.

The ACLS tachycardia algorithm is a step-by-step guide designed to help medical teams identify tachycardia and make quick decisions under pressure. It simplifies complex cardiac rhythm management into a clear plan that any member of a code team can follow. The main goal is to keep the heart pumping strongly and stop the patient from losing their pulse.
Once the algorithm is activated, you must immediately initiate a primary survey to secure the airway, support breathing, and assess circulation while establishing IV access and cardiac monitoring. Obtaining a 12-lead ECG and vital signs happens in parallel, as every data point informs the critical decision of whether the patient is hemodynamically stable or unstable.
The ACLS tachycardia algorithm follows a structured, step-by-step approach to rapidly assess and treat patients with dangerously fast heart rates. Each step builds on the last, guiding your team from initial pulse confirmation through rhythm identification to definitive treatment.
Before proceeding, palpate for a pulse for up to ten seconds. If pulse is not detected, immediately switch to the Cardiac Arrest Algorithm, as this protocol only applies to patients with a palpable pulse with a heart rate generally above 150 beats per minute. You must also determine if the rhythm is a primary arrhythmia or a normal physiologic response to fever, dehydration, pain, anxiety, or blood loss. If the patient is stable below 150 bpm, prioritize treating the underlying cause rather than the rhythm.
Your team must work in parallel to maintain a patent airway, provide supplemental oxygen if hypoxemic, and establish IV access. Attach a continuous cardiac monitor and pulse oximeter immediately, prioritizing a 12-lead ECG to accurately identify the rhythm and guide all subsequent treatment decisions.
Simultaneously, you must actively screen for reversible causes using the H’s and T’s framework, specifically ruling out hypoxemia and hypovolemia as primary reasons for the fast heart rate. Addressing these underlying triggers can often resolve the tachycardia without the need for aggressive medications or electrical therapy. If you are ever uncertain about the rhythm or the appropriate intervention, do not hesitate to seek expert consultation at any point during the algorithm.
It is important to identify if the patient has a stable or unstable tachycardia, as stability determines whether you pursue synchronized cardioversion or vagal/pharmacologic maneuvers. A patient is considered unstable if they show any of these five life-threatening signs:
If any of these are present, the patient needs immediate intervention. If they are alert with normal blood pressure and no chest pain, they are considered stable, which allows for a more methodical approach to medication and rhythm analysis.
After determining whether the patient is stable or unstable, the algorithm directs you into one of two distinct treatment pathways. Each pathway is driven entirely by the patient’s hemodynamic status, and choosing the wrong one can be dangerous. You should follow the appropriate pathway below based on your clinical assessment.
When a patient is unstable due to a fast heart rate, medications are rarely the first choice because they take too long to act and may further destabilize a patient whose cardiovascular system is already compromised. You must perform synchronized cardioversion immediately. This delivery of electricity is timed to the R-wave of the QRS complex to avoid delivering a shock during the vulnerable period of the T-wave, which could induce ventricular fibrillation.
When a patient is unstable, you must act fast. Synchronized cardioversion is the standard of care to restore a normal rhythm before the patient’s condition worsens.
If the patient is stable, the management strategy depends on the width of the QRS complex on the ECG. This systematic approach allows you to use vagal maneuvers or medications to control or convert the rhythm.
Narrow complex means the QRS duration is less than 0.12 seconds. For regular narrow rhythms like Supraventricular Tachycardia (SVT), start with vagal maneuvers like the Valsalva maneuver. If these fail, the primary medication is Adenosine. Give a 6mg rapid IV push followed by a 20mL saline flush. If the rhythm does not convert within one to two minutes, a second dose of 12mg can be given. If adenosine doesn’t work as well, try a beta-blocker or calcium channel blocker.
A wide complex rhythm, defined by a QRS duration greater than 0.12 seconds, is one of the most challenging arrhythmias to diagnose under pressure. Since distinguishing between ventricular tachycardia and SVT with aberrancy is often impossible from an ECG alone, you must always treat the rhythm as ventricular tachycardia if you are uncertain. Administering AV-nodal blocking agents to a patient in true VT is dangerous and can lead to rapid hemodynamic collapse.
For stable patients with an uncertain wide-complex origin, a rapid 6 mg IV push of adenosine can serve both a diagnostic and therapeutic role. If the rhythm converts to sinus, you have confirmed SVT with aberrancy. If there is no change, you should proceed with antiarrhythmic therapy. Never give adenosine to unstable wide-complex patients, as they require immediate electrical intervention instead.
Immediately reassess your patient following any electrical or pharmacological intervention by checking the monitor, re-evaluating vital signs, and confirming clinical status. If the tachycardia persists despite the initial treatment, you are managing a refractory rhythm that requires immediate escalation. For stable patients who fail to convert with medications, you should prepare for synchronized cardioversion. However, if a patient converts but then re-enters tachycardia, consider starting an antiarrhythmic maintenance infusion and seeking expert consultation.
Throughout this entire process, you must continue to investigate and treat any reversible underlying causes. The heart rhythm is unlikely to remain corrected if hypoxia or electrolyte imbalance remains unaddressed. Maintaining this dual focus on the rhythm and the cause is the key to achieving long-term stability for your patient.
Getting medications right is essential for successful tachycardia management. Precise preparation and administration techniques prevent treatment failure and protect your patient from avoidable harm during these critical cardiac events.
Carefully screen patients before prescribing beta-blockers (Metoprolol) or calcium channel blockers (Diltiazem), as both can worsen acute heart failure and cause severe bradycardia or heart block. Avoid beta-blockers in asthma patients and do not combine both drugs without specialist guidance.
Understanding the ACLS tachycardia algorithm is not just about passing a test but having the confidence to act when a patient’s life is on the line. By learning the critical divide between stable and unstable patients, you can provide the right intervention at the right time. Whether you are delivering a life-saving shock or administering precise medication doses, your systematic approach improves outcomes and prevents cardiac arrest.
If you are ready to sharpen your emergency response skills, CPR Lifeline provides hands-on training and updated 2025 AHA resources to help you stay prepared for any clinical scenario. Enroll in our ACLS certification or recertification courses today to gain the expertise you need to lead your team during an emergency situation.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
The ACLS tachycardia algorithm is a systematic, evidence-based treatment protocol for patients with heart rates exceeding 100 beats per minute. It guides healthcare providers through assessment and intervention based on whether the patient is hemodynamically stable or unstable.
Signs of unstable tachycardia include hypotension (systolic BP below 90 mmHg), acutely altered mental status, ischemic chest pain, or acute heart failure symptoms. These signs indicate the rapid heart rate is causing dangerous hemodynamic compromise requiring immediate intervention.
Synchronized cardioversion should be performed immediately when a tachycardic patient shows signs of instability. Do not delay for medications or further testing. The patient's unstable condition indicates the rhythm is life-threatening and requires urgent electrical intervention to restore effective cardiac output.
Start with vagal maneuvers like the Valsalva technique for stable supraventricular tachycardia. If vagal maneuvers fail, give adenosine 6 mg rapid IV push followed immediately by a 20 mL saline flush. Increase to 12 mg if the first dose does not convert the rhythm.
The main medications include adenosine for SVT, amiodarone and procainamide for wide complex tachycardia, and beta-blockers or calcium channel blockers like metoprolol and diltiazem for rate control. Medication choice depends on rhythm type and QRS width.
Use 50 to 100 joules for narrow complex regular tachycardia, 100 joules for wide complex regular tachycardia, and 120 to 200 joules biphasic for irregular narrow complex rhythms like atrial fibrillation. Always activate sync mode before delivering the shock.
Stable patients maintain adequate blood pressure, stay alert and oriented, have no chest pain, and show no heart failure signs. Unstable patients demonstrate hypotension, altered mental status, ischemic chest discomfort, or acute pulmonary edema from inadequate cardiac output.

Home | About Us | Classes | Locations | Blogs | FAQ’s | Group Training | Contact Us
Copyright © 2025 cprlifeline. All Rights Reserved. Powered by Splendour Group
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!