The ACLS stroke algorithm provides a systematic approach to identifying and treating suspected stroke patients. It’s part of Advanced Cardiovascular Life Support (ACLS) protocols developed and regularly updated by the American Heart Association. It is a clinical checklist that guides healthcare providers through critical decisions in the right sequence.
This algorithm includes everything from pre-hospital stroke recognition and emergency transport to in-hospital neurological assessment, brain imaging, and treatment decisions. It connects seamlessly with EMS, radiology departments, neurology teams, and intensive care units to create a coordinated chain of survival. New updates instructs CT imaging within 25 minutes and treatment decisions within 60 minutes, because 1.9 million neurons die every minute during a stroke, meeting these rapid targets is vital to preserving brain function.

The ACLS stroke algorithm is an evidence-based guide that helps medical teams make quick, life-saving decisions during a suspected stroke. This framework simplifies decades of neurological research into a clear roadmap, ensuring that every member of the stroke team can provide standardized, rapid intervention during critical cerebrovascular emergencies.
The primary goal is to minimize brain injury by restoring blood flow as quickly as possible. It prioritizes rapid symptom recognition, immediate imaging to differentiate stroke types, and timely reperfusion therapy for eligible patients. This structured protocol enables stroke teams to deliver critical interventions like tPA administration and mechanical thrombectomy within the therapeutic window, maximizing the chances of neurological recovery.
The ACLS Stroke Algorithm provides a structured, evidence-based sequence for managing adult stroke, emphasizing minimal delays in imaging and treatment. Here are the six definitive steps you must follow when a stroke is suspected.
You start by recognizing the warning signs using the primary recognition acronym, FAST or the BE-FAST acronym. It helps clinicians and first responders identify stroke symptoms and initiate urgent care. FAST or BE-Fast stands for Balance difficulties, Eyes vision loss, Facial drooping, Arm weakness, Speech difficulties, and Time to call emergency services.
As soon as you suspect a stroke, it is important to note the exact time symptoms began. If you don’t know when they started, record the last time the patient appeared normal, as this timestamp determines eligibility for time-sensitive treatments.
Immediately assess and manage the patient’s airway, breathing, and circulation and provide oxygen if needed. Perform a quick blood glucose check to rule out hypoglycemia, as it mimics stroke symptoms. Establish IV/IO access and notify the receiving hospital en route to ensure the stroke team is activated and prepared for the patient’s arrival.
Upon the patient’s arrival in the emergency department, a time-sensitive protocol begins. Within the first 10 minutes, the priority is to assess the patient rapidly. It includes checking vital signs, establishing a second IV line if necessary, and starting lab work, which should include glucose, CBC, coagulation panel, electrolytes, and cardiac markers. If the patient is hypoxemic, provide supplemental oxygen. Simultaneously, obtain a 12-lead ECG to rule out a cardiac cause, such as atrial fibrillation, and activate the stroke team. The patient must be sent for emergent brain imaging, as a non-contrast CT scan is required to determine if the stroke is ischemic or hemorrhagic. It must be completed within 25 minutes of arrival.
A focused neurological examination must be performed by a designated member of the stroke team within 25 minutes of the patient’s arrival. Most teams use the NIH Stroke Scale or the Canadian Neurological Scale to measure stroke severity. It works by scoring 15 specific functions, such as vision, language, and motor skills, to get a clear picture of the patient’s condition. At the same time, it is best to have someone gather a detailed history of the patient. Pinpoint the last known well time, assess their baseline function, and ask about any recent trauma. Be sure to note their medications, especially anticoagulants and antiplatelets. This clinical picture, combined with imaging, helps determine the safest and most effective treatment path.
The crucial step in the ACLS Stroke Algorithm is identifying the stroke type quickly. A CT scan should be reviewed within 45 minutes of the patient’s arrival, as it guides all further treatment decisions.
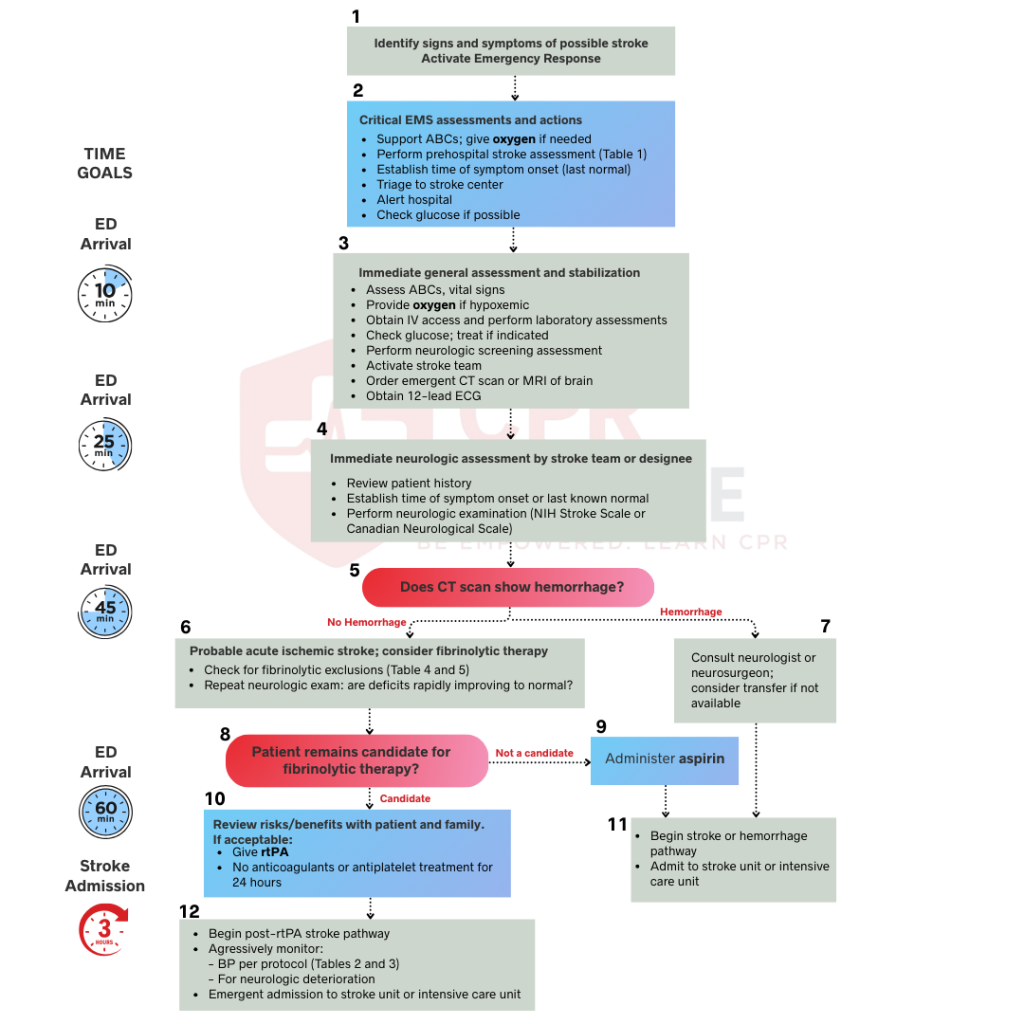
If the CT scan shows bleeding, the patient has a hemorrhagic stroke. This type of patient needs specialist intervention immediately. It is important to consult neurology and neurosurgery right away, as they determine the next steps. The patient may need surgery to stop the bleeding or relieve pressure on the brain.
You should admit the patient to the ICU for close monitoring and aggressive care. Watch for signs of worsening bleed, hydrocephalus, seizures, or any other complications. Remember not to give tPA, aspirin, or any blood thinners, as these medications will make the bleeding worse and can be fatal.
A CT scan showing no bleeding indicates a likely ischemic stroke, meaning a blood vessel in the brain is blocked. This diagnosis makes the patient a potential candidate for fibrinolytic therapy to dissolve the clot. Before administering tPA, you must carefully check for exclusion criteria such as a head injury or stroke within the past three months, a history of intracranial hemorrhage, blood pressure exceeding 185/110 mmHg, active internal bleeding, blood sugar below 50 mg/dL, or recent major surgery.
If none of these issues are present, you should repeat the neurologic exam to confirm that the stroke symptoms are persisting and ensure the patient remains medically stable for treatment. Once the stroke type is confirmed and consent is obtained from the patient and their family, you must move immediately to reperfusion therapy. For ischemic strokes, the treatment path depends on the time of onset and the location of the vessel blockage.
If the patient is eligible, initiate rtPA therapy within 1 hour of arrival and 3 to 4.5 hours of symptom onset.
If the patient is ineligible for fibrinolytics, administer 160 to 325 mg of aspirin (oral or rectal) to prevent further clotting. It reduces the risk of recurrent stroke in the acute phase. Give aspirin only after you have ruled out hemorrhagic stroke with imaging.
After tPA administration, admit the patient to a stroke unit or ICU within 3 hours of arrival. Check neuro status every 15 minutes during infusion, then every 30 minutes for 6 hours, then hourly until 24 hours post-treatment. Watch for severe headache, increased confusion, seizures, vomiting, or sudden worsening of symptoms. Maintain the blood pressure and avoid nasogastric tubes, urinary catheters, or arterial lines for 24 hours. Obtain a repeat head CT at 24 hours before starting any antiplatelet or anticoagulant medications.
For large artery blockages (e.g., MCA or ICA), arrange for a catheter-based clot removal by an interventional neuroradiologist. It should be performed within 6 hours after symptom onset in most patients and up to 24 hours in selected patients with large vessel occlusion, guided by imaging. This procedure works best for clots in large arteries like the middle cerebral artery or internal carotid artery. Some patients receive both tPA and mechanical thrombectomy if they meet criteria for both treatments.
Get rehabilitation started as soon as the patient is stable. Getting physical, occupational, and speech therapy involved early can help them recover the function they’ve lost. The goal is to get them up and moving as soon as it’s safe, because early mobilization leads to better outcomes. Work with the rehabilitation team to build an individualized plan.
The next critical focus is secondary prevention, which involves controlling blood pressure, managing diabetes, treating high cholesterol, and addressing modifiable lifestyle factors.
Medications play a critical role in stroke management, but their effectiveness depends entirely on proper patient selection and precise timing. The right medication administered within the therapeutic window can mean the difference between complete recovery and permanent disability.
Securing reliable IV access is essential for stroke medication delivery. Most therapies require central or large-bore peripheral access for rapid administration. For patient safety, two separate IV lines should be established. A secondary team member should perform an independent verification of the calculated dosage, followed by a clear, verbal announcement of the agent, dose, and route immediately before delivery. Blood pressure should be monitored throughout the duration of the infusion. To minimize the risk of bleeding, clinicians must strictly withhold all anticoagulant and antiplatelet agents for 24 hours following the completion of tPA treatment.
The ACLS stroke algorithm is built upon the “8 Ds,” a step-by-step guide designed to help medical teams make quick, life-saving decisions from the moment symptoms are detected until the patient is admitted for recovery.
While mastering the Stroke Algorithm on paper is essential, real-world success depends on speed and coordinated team execution. Because “time is brain,” practicing these procedures in high-pressure simulations ensures every second is saved, which significantly increases the survival chance of the patient.
Turning clinical guidelines into split-second action requires well-trained muscle memory rather than simple checklists. At CPR Lifeline, we provide official American Heart Association ACLS courses designed to help providers meet every critical time target accurately. Our flexible blended learning format allows you to complete an online curriculum at your own pace before attending a quick in-person skills session. You receive your AHA certification the same day via email after the completion of your course.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
Time is the most important factor in stroke treatment. Brain tissue dies rapidly during a stroke. Starting treatment within the first few hours dramatically improves outcomes. The faster you restore blood flow to the brain, the more brain tissue you save and the better the patient's recovery.
No, only ischemic stroke patients who meet specific criteria receive tPA. You must rule out bleeding with CT imaging first. Patients must arrive within the treatment window and have no contraindications like recent surgery, active bleeding, or very high blood pressure.
tPA must be administered by a licensed healthcare professional, typically under the guidance of a physician. A neurologist or stroke team confirms eligibility before administration. The medication is usually given in the emergency department or stroke unit by a nurse with specialized training.
If stroke symptoms start during sleep or the exact time is unknown, doctors call it a "wake-up stroke." It makes treatment harder because tPA must be given within a few hours of symptom onset. Doctors use special brain scans (like MRI or CT perfusion) to check if there is still brain tissue that can be saved. If the scan looks good, the patient may still receive treatment.
tPA is a medication given through an IV that dissolves blood clots. At the same time, endovascular therapy is a procedure where doctors physically remove larger clots from the brain’s blood vessels using a tiny tube. This procedure allows for a longer treatment window, and often both are used together.
No, aspirin should never be given before imaging confirms that the stroke is not hemorrhagic. Giving aspirin during a hemorrhagic stroke makes bleeding worse and leads to fatal complications. Always wait for imaging results before administering any antiplatelet or anticoagulant medications.
Warning signs include severe drowsiness or confusion, increased weakness or difficulty moving, trouble speaking, seizures, severe headache, vomiting, very high blood pressure, or changes in the eyes. These signs may mean the stroke is progressing or that bleeding is occurring in the brain. Report these symptoms immediately. The medical team must act quickly to prevent further damage.

Home | About Us | Classes | Locations | Blogs | FAQ’s | Group Training | Contact Us
Copyright © 2025 cprlifeline. All Rights Reserved. Powered by Splendour Group
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!