The ACLS cardiac arrest algorithm is the standardized framework that provides health care professionals with a structured approach to resuscitation efforts during cardiac arrest situations. This evidence-based protocol, developed and regularly updated by the American Heart Association, gives medical teams a clear roadmap for managing the critical emergency they may encounter.
Refinements have been made in the 2025 AHA guidelines based on the latest research to enhance resuscitation practices. It now includes a unified Chain of Survival that applies to all cardiac arrests regardless of age or location. There is also greater emphasis on physiologic monitoring during CPR, point-of-care ultrasound, and streamlined team approaches.

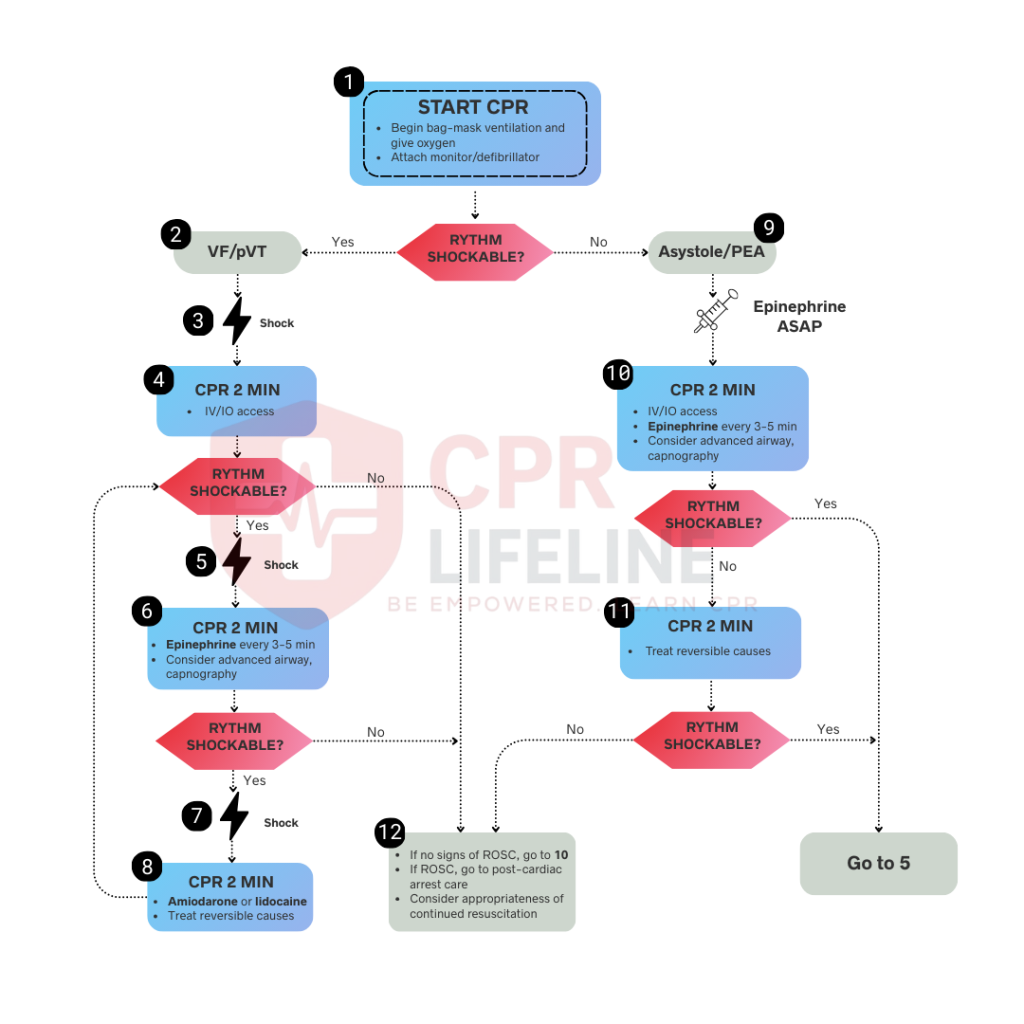
The ACLS cardiac arrest algorithm is a step-by-step evidence based guide designed to help medical teams make quick, life-saving decisions during a cardiac arrest.
It simplifies decades of medical research into a clear plan that anyone on a code team can follow during cardiac arrest.
The main goal of the ACLS Cardiac Arrest Algorithm is to improve survival rates and neurological outcomes during cardiac arrest by providing a systematic, evidence-based approach to resuscitation. It prioritizes high-quality CPR, early defibrillation for shockable rhythms, and rapid identification of reversible causes (the H’s and T’s). This structured protocol enables code teams to deliver timely interventions like epinephrine administration and advanced airway management, maximizing the chances of return of spontaneous circulation (ROSC).
High-quality CPR is the foundation of the ACLS cardiac arrest algorithm and must begin immediately once cardiac arrest is identified. You should begin chest compressions immediately at a rate of 100 to 120 compressions per minute with a depth of 2 to 2.4 inches in adults. Also, it is important to ensure full chest recoil between compressions to maintain oxygenated blood flow to the brain and vital organs.
Interruptions should be minimized and occur only for rhythm checks, defibrillation, or airway placement. The latest guidelines strongly advise utilizing physiologic monitoring to assess CPR quality and predict ROSC. The primary recommended tool is continuous waveform capnography (targeting ETCO2 >10–20 mmHg) for intubated patients. If an arterial line is in place, monitoring diastolic pressure (targeting >20 mmHg) is also reasonable.
Once high-quality CPR is underway, rhythm analysis becomes the critical decision point. After two minutes of CPR, pause compressions briefly for up to 10 seconds to assess the rhythm using a monitor or defibrillator and determine if it is shockable or non-shockable.
Shockable rhythms include ventricular fibrillation and pulseless ventricular tachycardia. Non-shockable rhythms are asystole and pulseless electrical activity (PEA). PEA was also previously called electromechanical dissociation and cannot include VF, VT, or asystole patterns.
1. Initial Defibrillation and Resume CPR
Charge the defibrillator while continuing compressions. Once ready, clearly announce and verify no one is touching the patient, then deliver the shock at 120 to 200 joules (biphasic). Immediately resume chest compressions without checking pulse or rhythm. Continue compressions for two minutes while establishing IV or IO access.
2. Second Rhythm Check and Epinephrine Administration
After 2 minutes, pause briefly to recheck the rhythm. If VF or pulseless VT persists, deliver the second shock immediately and resume compressions. During the next 2-minute cycle, give epinephrine 1 mg IV or IO and consider advanced airway placement. Repeat epinephrine every 3 to 5 minutes throughout resuscitation.
3. Antiarrhythmic Medication After Third Defibrillation
If the shockable rhythm still persists after three shocks, administer amiodarone 300 mg IV/IO to help stabilize the heart’s electrical activity. A second dose of amiodarone 150 mg can be followed if needed or Lidocaine may be considered. Continue the cycle of two-minute CPR, rhythm checks, and shocks until rhythm converts, ROSC occurs, or resuscitation efforts end. The latest guidelines note that antiarrhythmics may be more beneficial in witnessed arrests with early EMS response. Double sequential defibrillation is not recommended routinely for refractory cases due to lack of proven benefit.
Asystole and pulseless electrical activity carry lower survival rates than shockable rhythms but this approach is most helpful when the medical team can identify and treat the reversible cause that caused the cardiac arrest in the first place.
1. Continue High-Quality CPR and Establish Access
No defibrillation is needed for these types of rhythms. You should immediately continue high-quality chest compressions without interruption. Establish IV or IO access if not already present. Intraosseous access in the proximal tibia, distal tibia, or proximal humerus provides quick, reliable medication delivery.
2. Administer Epinephrine Immediately
Give epinephrine 1 mg as soon as IV or IO access is established, unlike shockable rhythms where it’s given after the second shock. Repeat epinephrine every 3 to 5 minutes throughout resuscitation. Continue CPR for two full minutes before checking rhythm again.
3. Identify and Treat Reversible Causes
Success depends heavily on identifying and correcting underlying causes. During CPR, quickly consider the H’s and T’s: hypovolemia, hypoxia, hydrogen ion (acidosis), hypokalemia, hyperkalemia, hypothermia, tension pneumothorax, tamponade, toxins, and thrombosis. Point-of-care ultrasound (POCUS) can help spot reversible causes like tamponade or thrombosis during brief pauses.
4. Reassess and Continue or Terminate
After 2 minutes, pause briefly to check rhythm. If non-shockable rhythm persists, resume CPR immediately and continue the cycle. If the rhythm converts to shockable, follow the shockable pathway with immediate defibrillation. Consider termination when no reversible causes are identified, and prolonged resuscitation attempts have failed. Most guidelines suggest at least 20 minutes of ACLS efforts before considering termination.
IV access is ideal, but intraosseous (IO) access remains a rapid, equally effective alternative for delivering medications directly into central circulation. For safety, designate one team member to handle pre-filled syringes and clearly announce the medication name, dose, and route.
Achieving ROSC (Return of Spontaneous Circulation) is a major milestone, but it marks a transition in care rather than the end of treatment. This phase is critical for preventing secondary brain injury and ensuring the best possible neurological outcome for the survivor.
Clinicians typically recognize the return of circulation through:
Once circulation is restored, the focus shifts to stabilizing vital organ functions through the following targets:
Manage blood pressure to ensure adequate organ perfusion. The goal is a Mean Arterial Pressure (MAP) of at least 65 mmHg. Use IV fluid boluses and vasopressor infusions (such as Dopamine or Norepinephrine) as needed.
For patients who remain comatose after ROSC, cooling the body to between 89.6°F (32°C) and 96.8°F (36°C) for at least 24 hours can significantly protect brain function.
Obtain an immediate 12-lead ECG. If ST-segment elevation is present, the patient requires urgent transfer to a cardiac catheterization lab, regardless of their level of consciousness.
Make sure to maintain oxygen saturation (SpO2) between 92% and 98%. Avoid excessive oxygen (hyperoxia) as it can cause oxidative stress to the brain which is recovering.
Learning the ACLS Cardiac Arrest Algorithm on paper provides a solid foundation, but mastering it in a real-life emergency requires hands-on practice. The ability to perform these procedures seamlessly within a team can significantly impact a patient’s survival rate.
At CPR Lifeline, we provide official American Heart Association (AHA) ACLS courses that give you practical skills and confidence to handle critical situations. Our programs are designed for busy medical professionals, with a flexible blended-learning format. You complete the online portion at your own pace and then come to one of our locations for a short, in-person skills check session. You’ll receive your AHA certification card the very same day via email.
If you’re ready to sharpen your life-saving skills and become an expert in advanced resuscitation, we encourage you to book an ACLS class with us. Become part of the thousands of healthcare providers who trust CPR Lifeline for their certification needs.
By submitting this form you agree to receive text messages at the provided number from CPR Lifeline LLC for appointment reminders. Message frequency varies, and standard message and data rates may apply. You have the right to OPT-OUT of receiving messages at any time. To OPT-OUT, reply “STOP” to any text message you receive from us. Reply HELP for assistance.
The ACLS cardiac arrest algorithm is a systematic, evidence-based protocol that guides medical teams through life-saving steps during cardiac arrest. It provides a clear framework for rhythm recognition, CPR, defibrillation, medications, and post-resuscitation care to maximize survival chances.
The two main pathways are shockable rhythms, which include VF and pulseless VT requiring immediate defibrillation, and non-shockable rhythms like asystole and PEA, which focus on high-quality CPR and finding reversible causes.
Give epinephrine 1 mg IV or IO every 3 to 5 minutes throughout the resuscitation. For non-shockable rhythms, administer it immediately. For shockable rhythms, give it after the second shock and continue at regular intervals.
Defibrillate immediately when you identify shockable rhythms like ventricular fibrillation or pulseless ventricular tachycardia. Charge the defibrillator during compressions, deliver the shock, and resume CPR immediately without checking for a pulse.
The H's are Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hypokalemia, Hyperkalemia, and Hypothermia. The Ts are Tension pneumothorax, Tamponade, Toxins, and Thrombosis (pulmonary or coronary). These represent reversible causes that require immediate treatment.
Chest compressions rate should be 100 to 120 per minute with a depth of 2 to 2.4 inches in adults. Allow complete chest recoil between compressions and minimize interruptions to less than ten seconds.
Just follow the manufacturer's suggested dose for biphasic machines, which is usually 120 to 200 joules for the first shock. Subsequent shocks should use the same or higher energy. If the recommended dose is unknown, use 200 joules.
Most guidelines suggest at least 20 minutes of high-quality ACLS efforts before considering termination. Continue longer if reversible causes are identified and treated, or if there are signs of improvement like increasing end-tidal CO2 levels.

Home | About Us | Classes | Locations | Blogs | FAQ’s | Group Training | Contact Us
Copyright © 2025 cprlifeline. All Rights Reserved. Powered by Splendour Group
#1. Select your Course, Location and Time
#2. Complete the AHA Online Training
#3. Perform the hands on skills check
#4. CONGRATS! You are certified!